Groin Spindle Cell Sarcoma
By Henning JE, Kazelka MH, Declue C, Bailey K, Ahmad N

Case Summary
An elderly patient with a history of a malignant kidney tumor and aortic aneurysm presented with chronic right inguinal pain. The patient denied recent trauma, swelling, and skin changes to the right groin, and they endorsed upper respiratory symptoms and a recent “popping” sensation in the right groin after coughing. Pelvic and abdominal CT scan raised concern for acute hemorrhage in the right groin. Coil embolization was successfully performed.
One month later, CT angiography demonstrated mild interval enlargement of the right inguinal canal region hematoma, consistent with a chronic hematoma, which characteristically expands following a hemorrhagic event.1
In this case, however, the patient also began experiencing lower abdominal discomfort, fatigue, and tachycardia. The growing mass and onset of new symptoms, some of which are common in cancer patients,2 prompted exploratory surgery, which demonstrated a right groin mass suspicious for malignancy. Biopsy and histopathology subsequently resulted in a diagnosis of malignant spindle cell neoplasm.
Imaging Findings
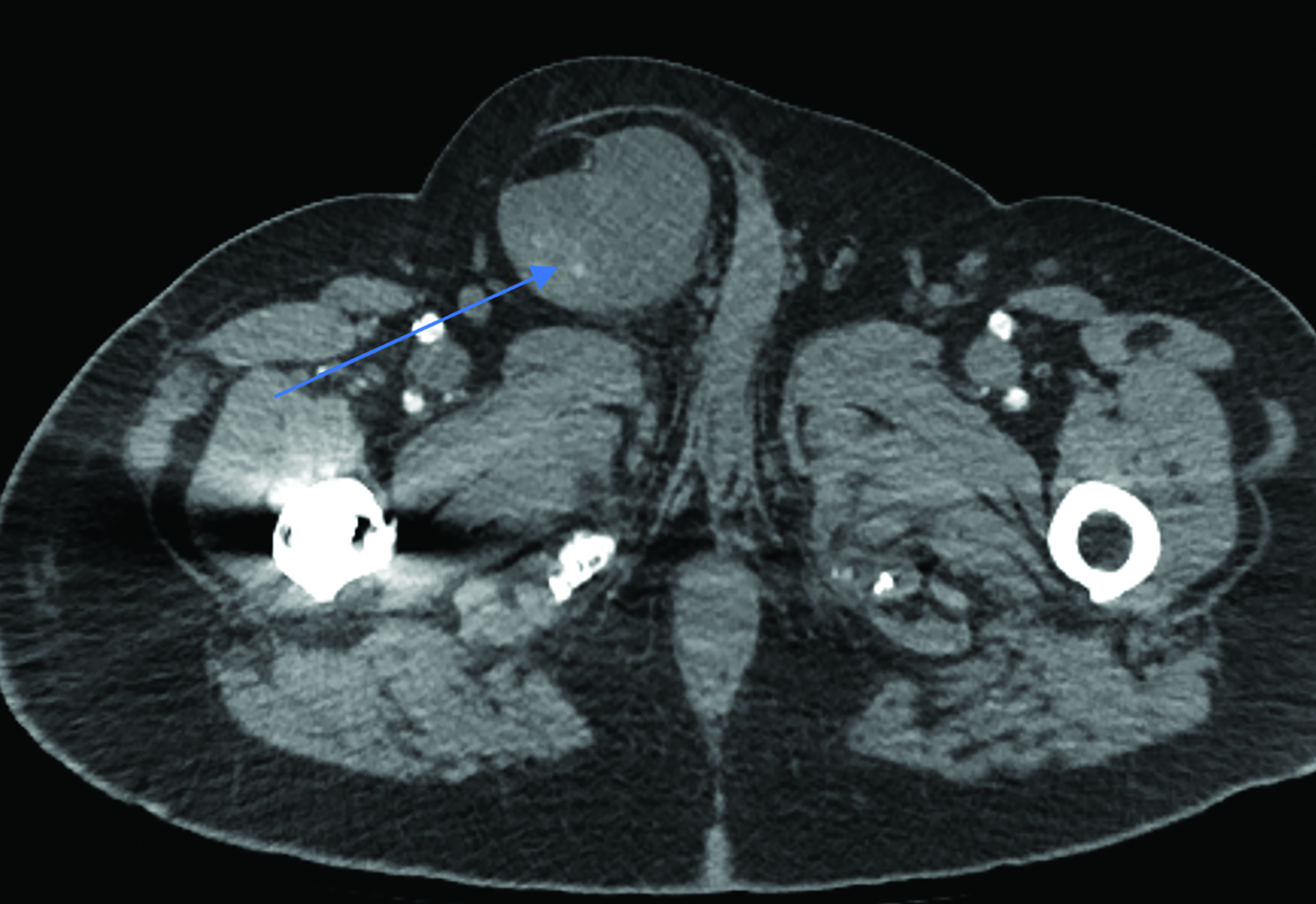
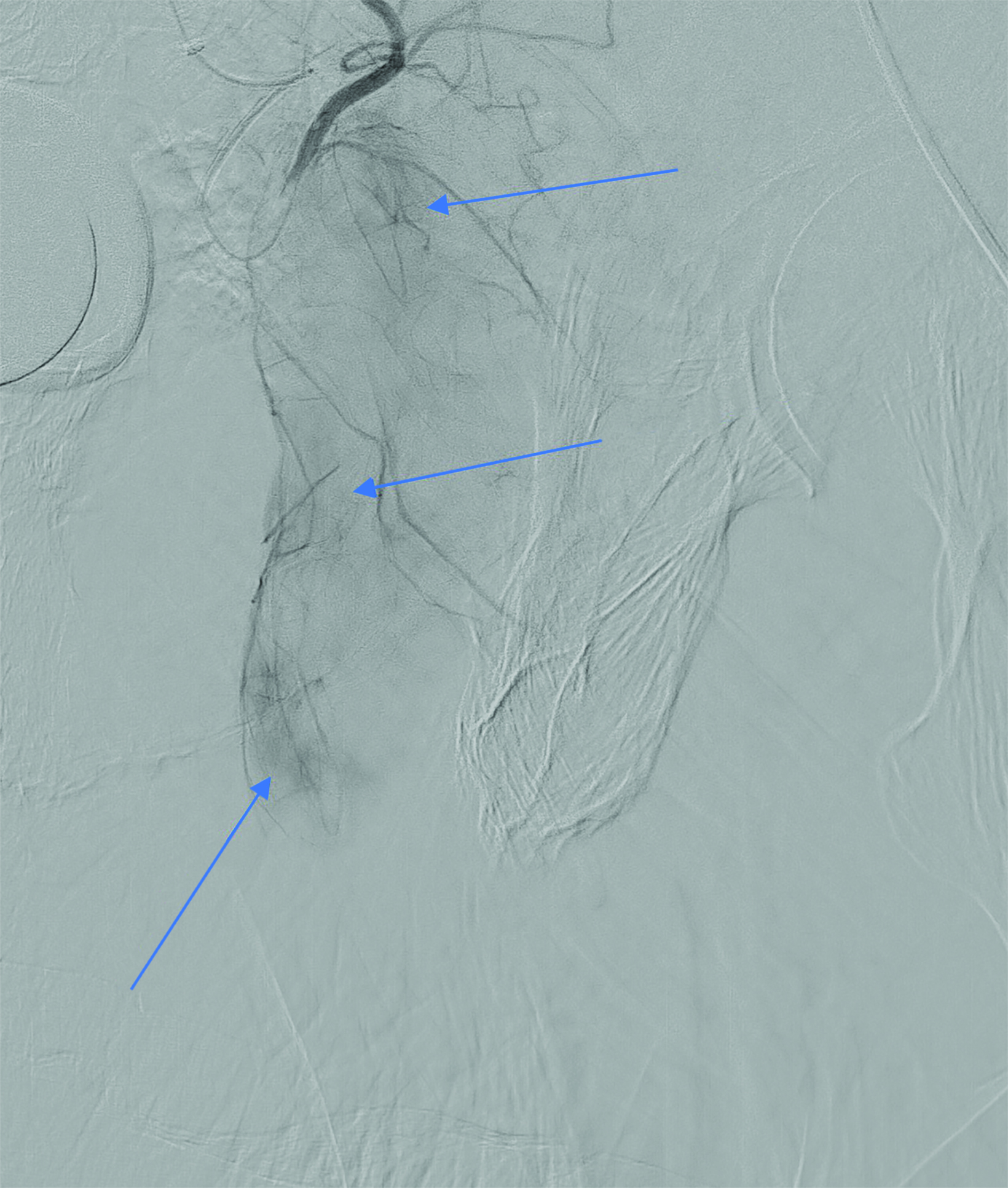
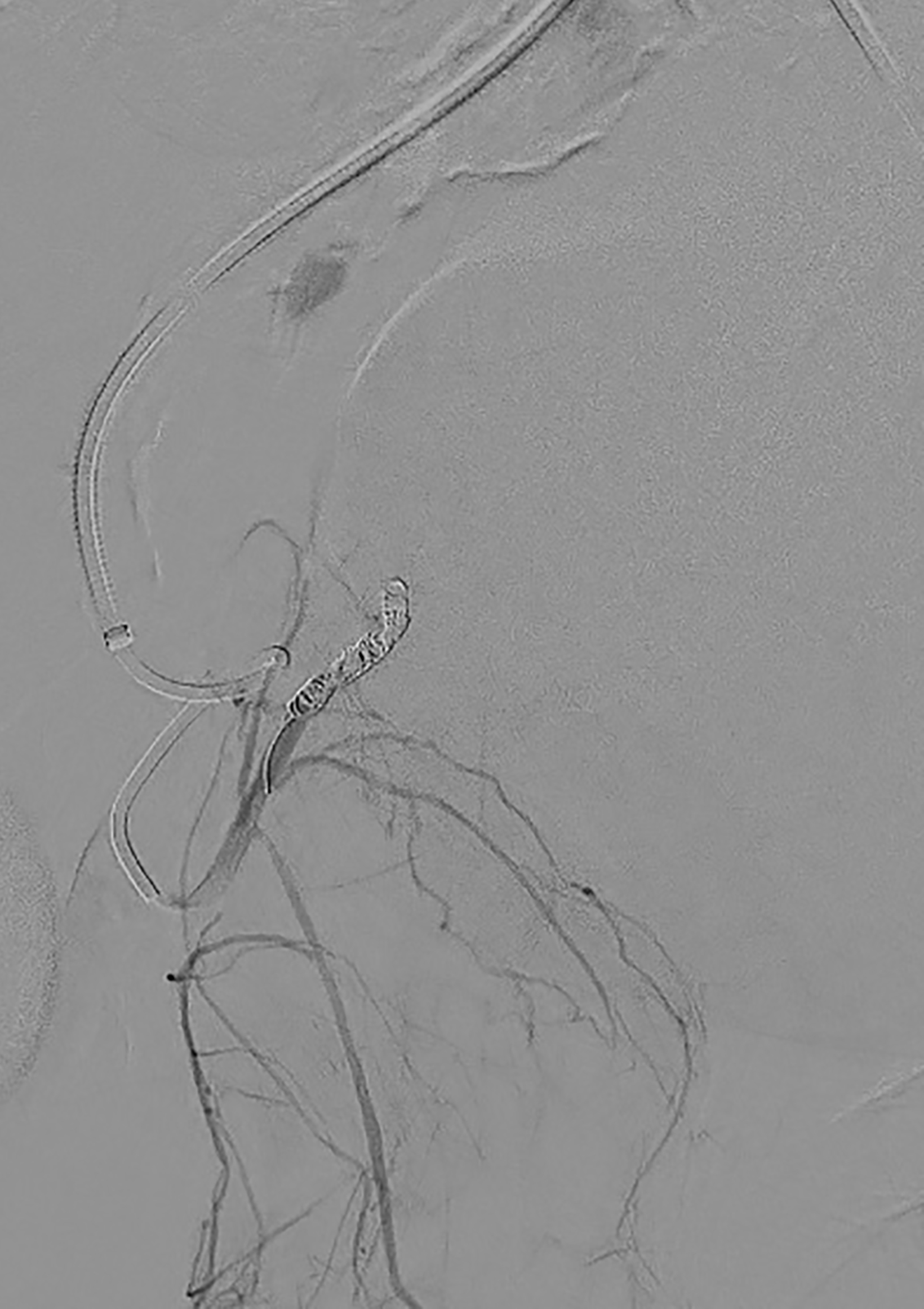
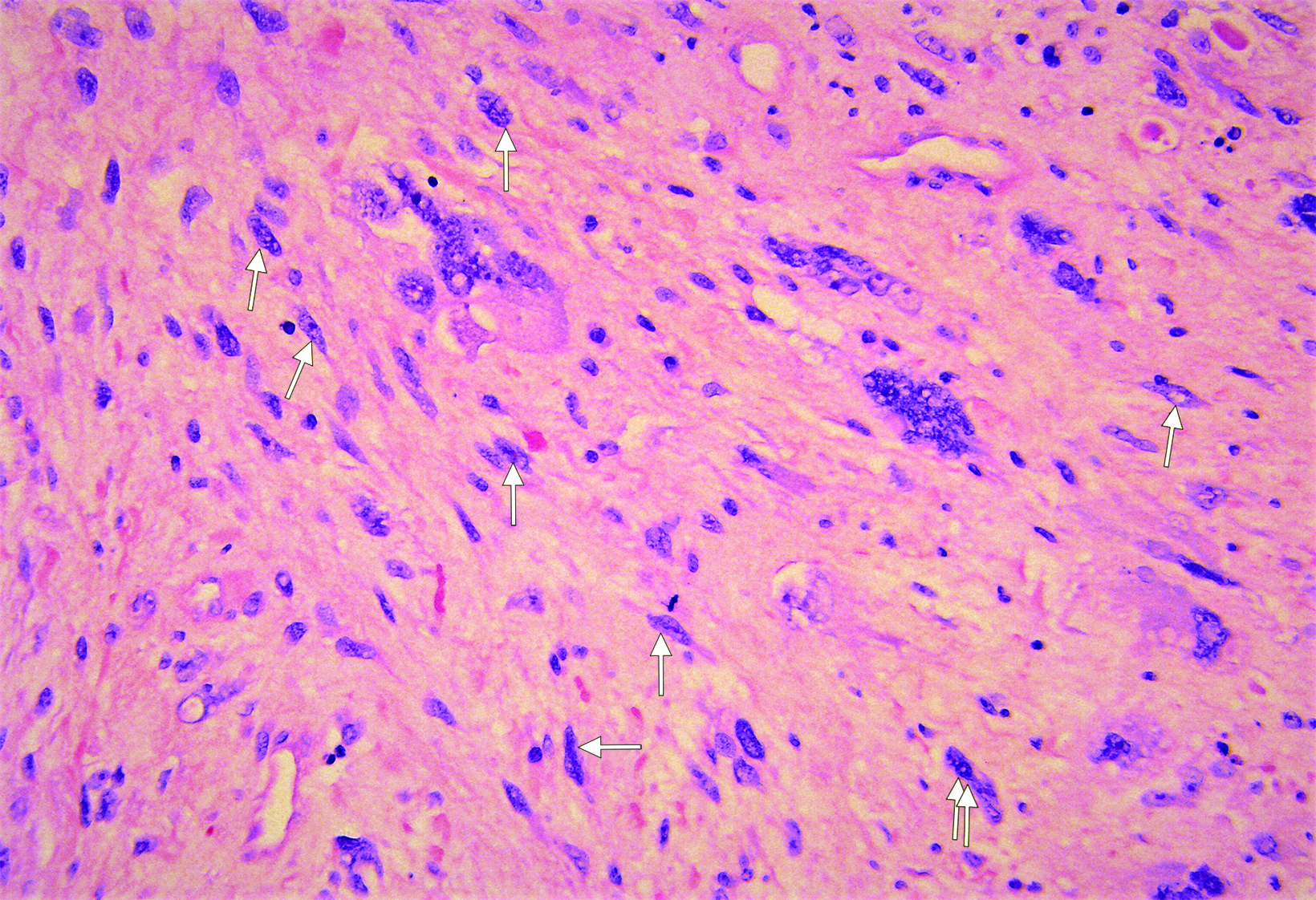
The initial abdominopelvic CT demonstrated a 10 cm × 5 cm × 6 cm heterogeneous collection with a blush (contrast pooling) appearing as an acute hemorrhage in the right inguinal canal (Figure 1). Catheter angiography prior to embolization demonstrated several irregular branches arising from the right inferior epigastric artery without contrast extravasation (Figure 2). One month postembolization, abdominopelvic CT revealed mild interval enlargement of the right inguinal canal region mass to 14.7 cm (Figure 3). Biopsy was performed (Figure 4).
Diagnosis
Malignant spindle cell sarcoma
Discussion
We present an unusual occurrence of a right groin spindle cell sarcoma disguised as a hematoma. Spindle cell sarcomas are a rare and heterogeneous type of soft-tissue sarcoma.3 They arise from layers of connective tissue and may occur in any anatomical location, including soft tissue, bone, and viscera.4 Given the heterogeneity of soft-tissue sarcomas, the clinical presentation is not well characterized. Owing to this obscurity, collections in the inguinal region can be mistaken for hematomas on imaging modalities such as ultrasound.5 In these cases of uncertainty, follow up and/or contrast-enhanced imaging plays an important role in correct diagnosis.
In most settings a metastatic inguinal neoplasm is an unlikely explanation for inguinal pain or mass. More probable causes include inguinal hernia, hydrocele, abscess, and hematoma.6 Visual and physical examination, however, can lower the probability of hernia, which presents as a bulge in the inguinal region.6 The absence of recent trauma, swelling, and skin changes of the right groin also reduce the likelihood of hernia.6
An effective tool for diagnosing the cause of inguinal pain, CT can typically distinguish among abdominal wall masses, tumors, hematomas, and unsuspected hernias.7 In this case, CT revealed a heterogeneous collection, as well as what was thought to be contrast extravasation, which may indicate active bleeding in the area.8
Given the concerns about bleeding, catheter angiography and coil embolization were performed. The procedure is indicated in cases of suspected active arterial hemorrhage to identify and occlude blood vessels and stop the bleeding.9
Conclusion
Malignant spindle cell sarcoma in the inguinal region is rare and may be missed because it can present with signs and symptoms that overlap with a groin hematoma. Imaging is essential to accurate diagnosis.
References
- Manenti G, Cavallo AU, Marsico S, et al. Chronic expanding hematoma of the left flank mimicking a soft-tissue neoplasm. Radiol Case Rep. 2017;12(4):801-806. doi: 10.1016/j.radcr.2017.07.019
- Cleeland CS. Cancer-related symptoms. Semin Radiat Oncol. 2000; 10(3):175-90. doi: 10.1053/srao.2000.6590
- Panthi S, Poudel S, Khanal N, et al. Spindle cell sarcoma: a case report of diagnostic and therapeutic quandary in a low resource setting. J Surg Case Rep. 2022 Jan 21; 2022(1):rjab612. doi: 10.1093/jscr/rjab612. PMID: 35079340.
- Feng L, Wang M, Yibulayin F, Zhang H, Yang YL, Ren F, Wushou A. Spindle cell sarcoma: a SEER population-based analysis. Sci Rep. 2018; 8(1): 5024. doi: 10.1038/s41598-018-23145-4
- Vodanovich DA, M Choong PF. Soft-tissue sarcomas. Indian J Orthop. 2018; 52(1):35-44. doi: 10.4103/ortho.IJOrtho_220_17
- Hammoud M, Gerken J. Inguinal hernia. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Available at: https://www.ncbi.nlm.nih.gov/ books/NBK513332/
- Lee GH, Cohen AJ. CT imaging of abdominal hernias. AJR Am J Roentgenol. 1993; 161(6):1209-13. doi: 10.2214/ajr.161.6.8249727
- Godt J C, Eken T, Schulz A, et al. Do we really need the arterial phase on CT in pelvic trauma patients? Emerg Radiol. 2021;28:37–46. doi: https://doi.org/10.1007/ s10140-020-01820-2
- Lopera JE. Embolization in trauma: principles and techniques. Semin Intervent Radiol. 2010; 27(1):14-28. doi: 10.1055/s-0030-1247885