Case Review: Heterotaxy syndrome with polysplenia

Click here to view and interact with the DICOM images for this case in the Exa-PACS zero foot print viewer provided by Viztek.
Case Summary
A middle-aged female presented to the hospital with hematuria.
Imaging Findings
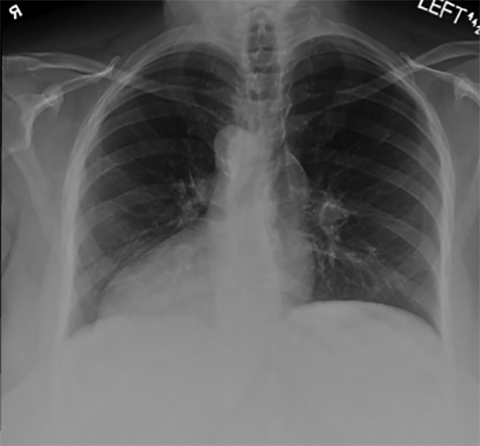
The patient’s admission chest radiograph demonstrated dextrocardia (Figure 1). The patient received a CT scan of the abdomen and pelvis, which did not demonstrate abnormalities to explain her symptoms. However, there were several abnormalities consistent with heterotaxy syndrome with polysplenia. Two years later, she received a CT of the chest for evaluation of a pulmonary nodule, which demonstrated additional findings consistent with heterotaxy syndrome.
The cardiovascular system demonstrated a right-sided aortic arch with a mirror-image, 3-vessel branching pattern. The main pulmonary artery arose from the right of the aorta. The patient exhibited dextrocardia, although no other CT evidence for cardiac anomaly was present. There was a left-sided inferior vena cava without a hepatic segment. The inferior vena cava drained into the right atrium via hemiazygos continuation.
The pulmonary system demonstrated bilateral left-sidedness, as both lungs were divided into upper and lower lobes. Neither lung demonstrated a minor fissure or middle lobe. Both main bronchi were hyparterial, meaning that each bronchus passed inferior to its corresponding main pulmonary artery.
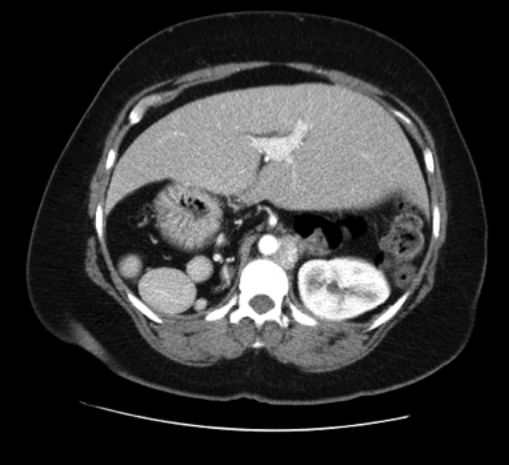
In the gastrointestinal system, there was a midline liver with a more prominent left lobe. The stomach was right-sided, with multiple right-sided spleens visualized adjacent to the greater curvature (Figure 2).
Diagnosis
Heterotaxy syndrome with polysplenia
Discussion
Situs solitus describes the normal orientation of organs with respect to the midline. In situs inversus, the organs are in mirror-image orientation compared to situs solitus. Situs ambiguous or heterotaxy describes an orientation of the organs that does not conform to either situs solitus or inversus. Heterotaxy syndromes are divided into bilateral right-sidedness, or asplenic heterotaxy, and bilateral left-sidedness, or polysplenic heterotaxy.
This patient’s CT demonstrated heterotaxy syndrome with bilateral left-sidedness. The constellation of findings in this syndrome also has been called situs ambiguous with polysplenia or left isomerism. There are no fixed characteristics or pathognomonic features in this syndrome. Patients can have levocardia or dextrocardia, with or without additional cardiac anomalies. Both lungs are bilobed and the bronchi are hyparterial, as seen in this patient. Some patients exhibit normal abdominal situs or a single spleen. Most patients have multiple spleens, as did this patient. The liver and gallbladder can be midline or right-sided. The inferior vena cava is often interrupted with azygos or hemiazygos continuation.1
Most patients with heterotaxy syndrome with polysplenia die by age 5, usually due to severe cardiac anomalies.2 An estimated 5-10% of patients, such as the patient presented here, have normal hearts or mild cardiac defects and demonstrate no symptoms.3
Heterotaxy syndrome with polysplenia is a congenital syndrome that is usually diagnosed in early childhood due to the manifestations of severe cardiac anomalies, which are often part of the syndrome, although cardiac anomalies are less common and complex in polysplenia than in asplenia.4 If there are no cardiac anomalies, the syndrome often goes undiagnosed until imaging is obtained for an unrelated reason in adulthood.5 Heterotaxy syndrome with polysplenia is more common in females.4 Genetic studies have found that heterotaxy syndromes likely exhibit multifactorial inheritance.6
A case review of 23 patients with heterotaxy syndrome with polysplenia demonstrated 19 cases with azygos or hemiazygos continuation of the inferior vena cava, all of which lacked a hepatic segment of the inferior vena cava. Only two cases demonstrated dextrocardia. Thirteen of the 23 cases demonstrated right-sided spleens. The case review also discussed short pancreas and malrotation in some patients, neither of which were visualized in the case presented here.5
Conclusion
Heterotaxy syndrome with polysplenia presents uniquely on radiography, and physicians should consider the imaging findings discussed in this case when forming a diagnosis. This study presents common findings associated with heterotaxy syndrome.
References
- Fulcher AS, Turner MA. Abdominal manifestations of situs anomalies in adults. Radiographics. 2002; 22:1439-1456.
- Peoples WM, Moller JH, Edwards JE. Polysplenia: A review of 146 cases. Pediatr Cardiol. 1983;4:129–137.
- Winer-Muram HT, Tonkin ILD. The spectrum of heterotaxic syndromes. Radiol Clin North Am.1989; 27:1147–1170.
- Applegate KE, Goske MJ, Pierce G, Murphy D. Situs revisited: Imaging of the heterotaxy syndrome. Radiographics.1999;19:837-852.
- Gayer G, Apter S, Jonas T, et al. Polysplenia syndrome detected in adulthood: Report of eight cases and review of the literature. Abdom Imaging 1999; 21:178-184.
- Niikawa N, Kohsaka S, Mizumoto M, Hamada I, Kajii T. Familial clustering of situs inversus totalis, and asplenia and polysplenia syndromes. Am J Med Genet. 1983;16:43-47.