Interventional Radiological Case: Hemorrhagic renal angiomyolipoma

CASE SUMMARY
A 63-year-old female patient with history of end-stage renal disease (ESRD) and tuberous sclerosis presented to the emergency department (ED) with right flank pain.
IMAGING FINDINGS
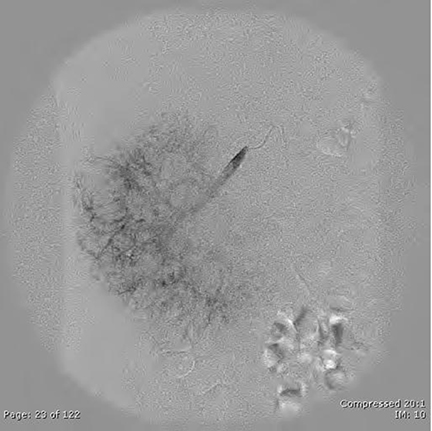
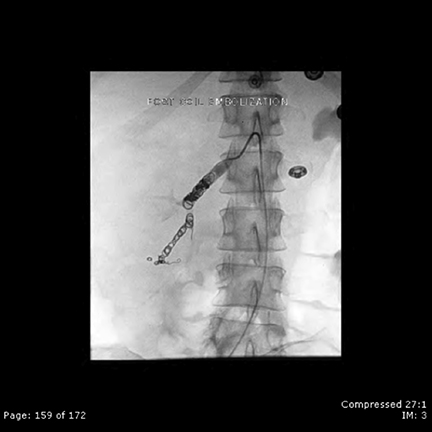
A computed tomography (CT) scan in the ED (Figure 1) revealed a new hemorrhagic mass in the upper pole of the right kidney. Three days after initial presentation, the patient’s hemoglobin levels fell by 3 units, and she was brought to IR for emergent embolization (Figures 2 and 3).
DIAGNOSIS
Hemorrhagic renal angiomyolipoma
There is a high-attenuation mass in the upper pole of the right kidney consistent with a hemorrhagic lesion. The differential diagnosis includes hemorrhage from an angiomyolipoma, renal cell carcinoma, or a metastatic lesion. The presence of bilateral fat-containing renal masses as well as a history of tuberous sclerosis make hemorrhagic renal angiomyolipoma the most likely diagnosis.
DISCUSSION
Tuberous sclerosis is an autosomal-dominant disease with variable penetrance that affects approximately 40,000 individuals in theUnited States and 2 million people worldwide. There are 2 abnormal genes associated with tuberous sclerosis, the TSC1 gene on chromosome Q19 and the TSC2 gene located on chromosome P16. These genes have an important role in tumor suppression. The classic triad of tuberous sclerosis consists of adenoma sebaceum, seizures, and mental retardation, but is only seen in one-third of patients.Major features of tuberous sclerosis include facial angiofibromas, cortical tubers, subependmal nodules, giant cell astrocytomas, cardiac rhabdomyomas, lymphagniomyomatosis, and renal angiomyolipomas.1
Angiomyolipomas (AML) are benign hamartomatous lesions composed of vessels, smooth muscle, and adipose tissue. Although80% are sporadic and solitary, 20% are multiple and associated with syndromes such as tuberous sclerosis. These lesions are generally benign except for the rare epitheliod subtype. Vessels associated with AMLs are dysplastic in nature and therefore predisposed to aneurysmal dilatation and hemorrhage, particularly when an AML is >4 cm. Therefore, embolization of lesions >4 cm is recommended.2. When there is spontaneous hemorrhage of AMLs, also known as Wunderlich’s syndrome, management options include conservative management, embolization, and nephrectomy depending on hemodynamic considerations. In the above mentioned case, the patient was actively bleeding and, therefore, could not be treated conservatively. Her hemodynamic status was stable enough to avoid surgical nephrectomy, and thus, she was an ideal patient for embolization.
CONCLUSION
Bilateral angiomyolipomas are very common in patients with tuberous sclerosis.When hemorrhage is noted or when they are >4 cm,embolization is recommended.
REFERENCES
- Castillo M. Neuroradiology: Core Curriculum. 1st ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002.
- Roth CG. Fundamentals of body MRI. Philadelphia, PA: Elsevier Saunders; 2012.