Right renal vein varix

Right renal vein varix
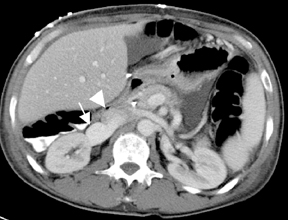
Findings
Computed tomography (CT) demonstrated a focal enhancing ovoid density adjacent to the right renal hilum continuous with the right renal vein. It had an enhancement pattern similar to that of the right renal vein.
Discussion
A frequent incidental finding, renal varices can be idiopathic or associated with either renal vein thrombosis, obstruction, or congenital anomalies of inferior vena cava, as well as azygous or portal hypertension.1,2 Idiopathic renal varices demonstrate left predominance, with an incidence of 6% to 10% in renal donors on phlebography.1,3 The etiology of left predominance in idiopathic cases has been postulated to be stretching of the renal vein over the aorta and compression between the superior mesenteric artery (SMA) and the aorta, known as the nutcracker phenomenon.1,4 In addition, extensive collaterals from other organs and weakness of the vein wall may be contributing factors.1 Furthermore, the absence of gonadal vein valves and abnormal collaterals between the renal and gonadal veins have been suggested as contributing factors.2 In 31% of renal vein varix there is associated saphenous vein varicosity.
Extrarenal varices are more common than intrarenal.5 The latter may have calcifications and can simulate renal masses, especially if thrombosed.5,6 The differential of renal varix includes renal or urothelial neoplasm, hemangioma, blood clots, pyelo-ureteritis cystica, leukoplakia, tuberculosis, and radiolucent calculi.4,5 Failure to recognize this characteristic appearance may lead to unnecessary nephrectomy.6
Although the excretory urogram may demonstrate external compression of the renal pelvis or proximal ureter by the varix, phlebography with or without epinephrine is the historic diagnostic modality of choice.1,6 However, contrast enhanced CT or magnetic resonance imaging (MRI) detect renal varices noninvasively.5 CT demonstrates attenuation matching and is continuous with that of renal vein on pre- and post-contrast images.5 MRI demonstrates signal voids on the axial spin echo and T2-weighted images, and high signal on the modified gradient echo and phase contrast with gadolinium imaging, similar to that in other veins.5 The sagittal plane is especially useful for evaluation of nutcracker syndrome. In these patients, MRI demonstrates the acute take-off angle of the SMA from the aorta.7 It could be used to diagnose this condition noninvasively, rather than demonstrating the pressure gradient between the renal vein and the IVC during venography.2 In addition, Technetium-99m red blood cells have been used to demonstrate pooling in a case of renal varix caused by hematuria.3
Pain with renal varices is extremely rare. Varices are typically asymptomatic and only infrequently associated with hematuria.5,8 Whether renal varices actually cause hematuria is controversial.5 Nevertheless, surgical ligation or embolization are frequently used in patients with hematuria and/or pain but no other explanation.5 The transposition of the left renal vein to a more caudal location has been successfully used in nutcracker syndrome.7 Other complications include partial or complete obstruction and renal stone formation.5
Conclusion
Renal vein varices are a frequent incidental finding on CT or MRI. Renal varices may mimic renal masses especially on noncontrast CT scans. The continuity with renal vein and similarity to vein appearance on all imaging modalities are important differentiating factors. Complications are rare, and include hematuria, obstruction, and stone formation. Surgical ligation or embolization may be used to treat varices associated with pain or hematuria.
- Beckmann CF, Abrams HL. Idiopathic renal vein varices: Incidence and significance. Radiology. 1982;143(3):649-652.
- Weiner SN, Bernstein RG, Morehouse H, Golden RA. Hematuria secondary to left peripelvic and gonadal vein varices. Urology. 1983; 22(1):81-84.
- Rendak I, Pison C, Drouin G. Demonstration of renal varices using technetium-99m red blood cells in the investigation of recurrent macroscopic hematuria. Clin Nucl Med. 1987;12(11):861-863.
- Trambert JJ, Rabin AM, Weiss KL, Tein AB. Pericaliceal varices due to the nutcracker phenomenon. AJR Am J Roentgenol. 1990;154(2):305-306.
- Deibler AR, Nadig SN, Curry N, Bissada NK, Hull GW. Intrarenal varix presenting as an enhancing renal mass with calcifications. J Urol. 2001;166(3):997-998.
- Curry NS, Frangos DN, Stanley JH. Thrombosed right renal vein varix simulating a renal pelvic mass. Urol Radiol. 1987;9(1):36-38.
- Hohenfellner M, Steinbach F, Schultz-Lampel D, et al. The nutcracker syndrome: New aspects of pathophysiology, diagnosis and treatment. J Urol. 1991;146(3):685-688.
- Nielsen PT, Nielsen SM. Idiopathic renal vein varicosities. Presentation of two cases and a brief review of the literature. Scand J Urol Nephrol. 1984;18(1):91-95.