Traumatic Cribriform Plate Defect Following Self-administered COVID-19 Nasal Swab Test



Case Summary
A middle-aged patient presented with mild, typical symptoms of COVID-19 that included alterations in smell and taste, fever, and a mild cough. COVID-19 was diagnosed after a provider-performed nasal swab, and hospitalization was not required. A few days later, the patient performed a self-administered COVID nasal swab for retesting. Approximately two days later, the patient developed a severe headache and noticed clear rhinorrhea. They presented to the emergency department with a fever of 102°F.
Imaging Findings
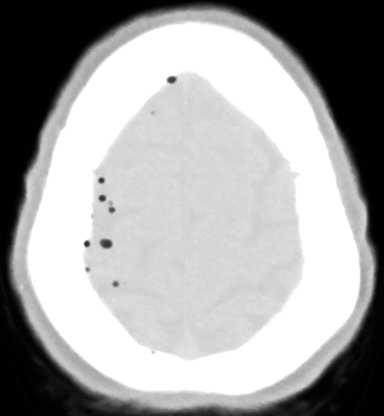
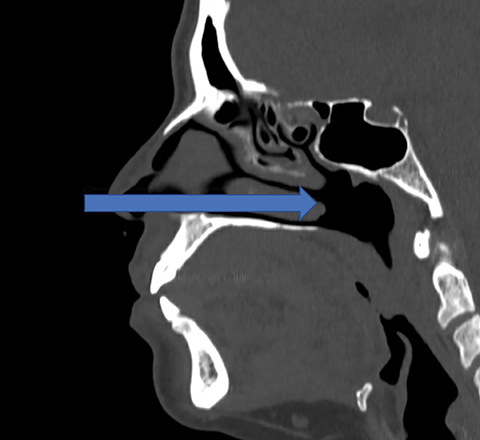
A CT scan of the head showed pneumocephalus exclusively on the right side (Figure 1). A sagittal image revealed a defect in the cribriform plate (Figure 2). A cephalocele was seen herniating through the defect (Figure 3).
Diagnosis
Traumatic encephalocele and CSF leak caused by self-administered COVID-19 nasal swab.
Discussion
The current gold standard for SARS-CoV-2 testing remains reverse transcription polymerase chain reaction (RT-PCR) with a nasopharyngeal or nasal swab.1 At the time of the patient’s presentation, approximately 80 million tests had been performed in the US, according to the Centers for Disease Control and Prevention (CDC).2 With the dramatic increase in demand for COVID-19 tests, there have been several responses to increase availability, including drive-through testing, and self-performed tests. Although the risks of nasal swab testing are generally low, the risk of tissue injury is understandably increased when the tests are self-administered by a minimally instructed individual.
There is a common misconception, likely owing to the upward angle of the external nose, that the path from the nostril to the nasopharynx angles upward.3 However, the true path is nearly flat, parallel to the ground in a patient sitting upright.4 The proper trajectory of a nasal swab is demonstrated in Figure 4. Given the patient’s cribriform plate fracture site, the trajectory they used can be inferred and is shown in Figure 5, which would be the path used by an individual holding the misconception that the proper route angles upward. With little training provided to individuals, a large portion of self-administered tests are likely performed incorrectly. Had our patient performed the nasal swab at the appropriate angle, the cribriform plate would not have been impacted and the patient’s hospital course could have been prevented.
We have been able to find only one other reported case of a traumatic CSF leak from a COVID-19 nasal swab test.5 This case was provider performed, however, and the patient was found to have a large, preexisting encephalocele on imaging performed prior to the nasal swab, putting the patient at a much greater risk of iatrogenic injury.
Our patient was started on broad spectrum antibiotics for meningitis coverage, and the otolaryngology (ENT) service was consulted for management of the patient’s skull base defect. The ENT surgeon determined that the patient was a candidate for endoscopic endonasal resection and repair. During the procedure, the defect through the lateral process of the right cribriform plate and the encephalocele herniating through the defect were confirmed. The CSF leak was successfully repaired using a free mucosal graft from the right middle turbinate. The patient was discharged with instructions to complete 2 weeks of IV antibiotics. They reported being asymptomatic with complete resolution of both headaches and CSF rhinorrhea at follow-up.
Conclusion
Although generally viewed as safe, nasal swab testing is not without risk. Individuals performing self-administered tests with minimal training are understandably at a much higher risk of injury than those tested by well-trained medical staff. This case demonstrates the possibility of intracranial injury when a test is improperly performed, with potentially devastating consequences, including CSF leaks, encephaloceles, and meningitis. At-home tests should include materials such as written explanations, illustrations, photographs, and/or video to demonstrate proper technique and provide for e safe and adequate testing.
References
- Interim Guidance for Rapid Antigen Testing for SARS-CoV-2. Published 2020. https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/antigen-tests-guidelines.html. Accessed October 3, 2020.
- Previous U.S. Viral Testing Data. Centers for Disease Control and Prevention. Published 2020. https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/previous-testing-in-us.html. Accessed October 3, 2020.
- Higgins TS, Wu AW, Ting JY. SARS-CoV-2 Nasopharyngeal swab testing—false-negative results from a pervasive anatomical misconception. JAMA Otolaryngol Head Neck Surg. Published online September 17, 2020. doi:10.1001/jamaoto.2020.2946.
- How to Obtain a Nasopharyngeal Swab Specimen. New Engl J Med. Published online. https://www.nejm.org/doi/full/10.1056/NEJMvcm2010260. Accessed October 3, 2020.
- Sullivan CB, Schwalje AT, Jensen M, et al. Cerebrospinal fluid leak after nasal swab testing for coronavirus disease 2019. JAMA Otolaryngol Head Neck Surg. Published online Oct.1, 2020. doi:10.1001/jamaoto.2020.3579.
Baylor University Medical Center, Dallas, TX