Cleidocranial Dysplasia
Images

Case Summary
An adolescent presented for evaluation of short stature and a prominent forehead. On examination, the patient had brachycephaly with frontal bossing and a prominent depression at the expected location of the metopic suture. Other findings on physical examination were wide-set eyes, down-sloping shoulders, a few supernumerary teeth, and tapering digits. Similar findings and short height were also observed in his father.
Imaging Findings
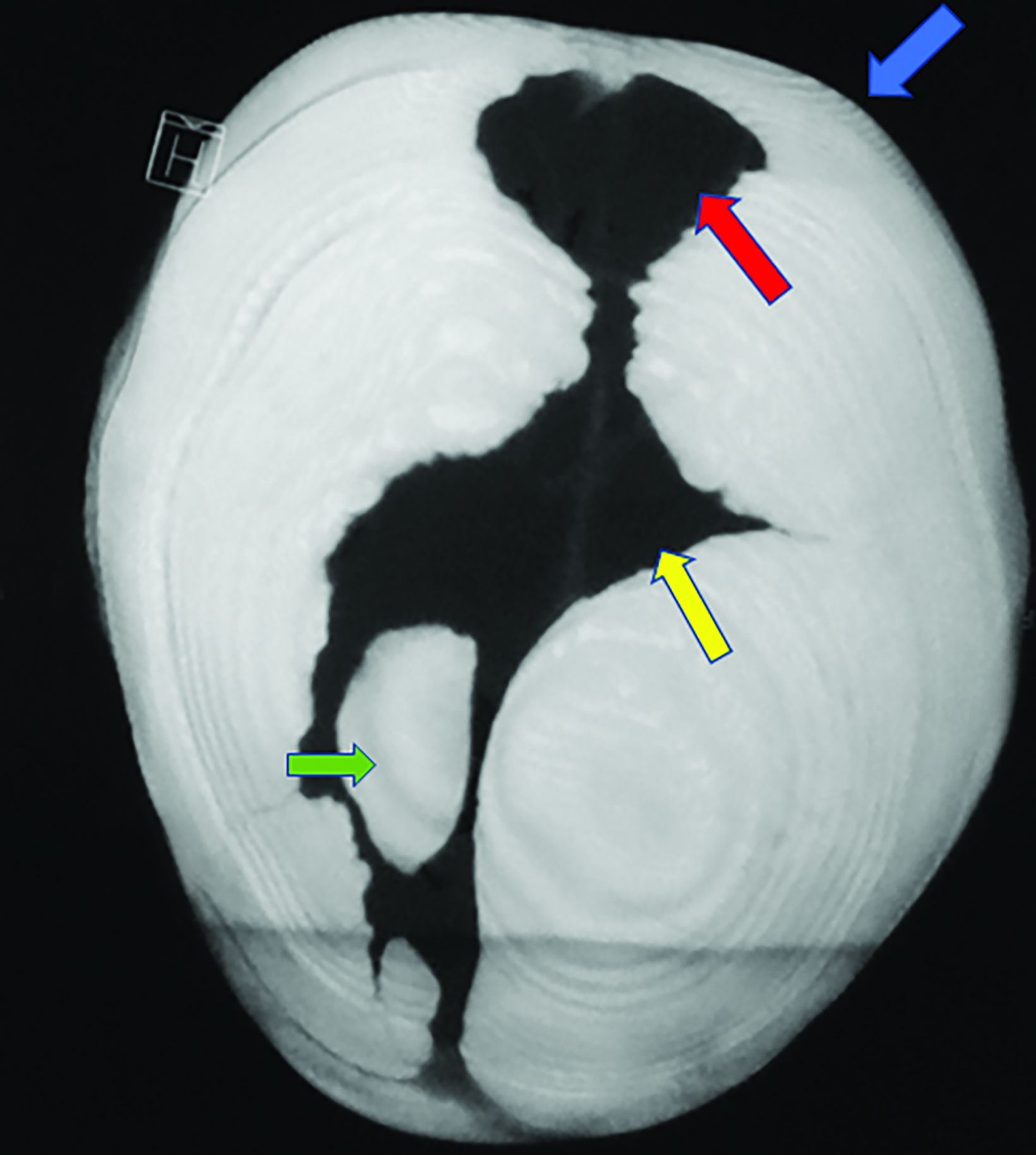
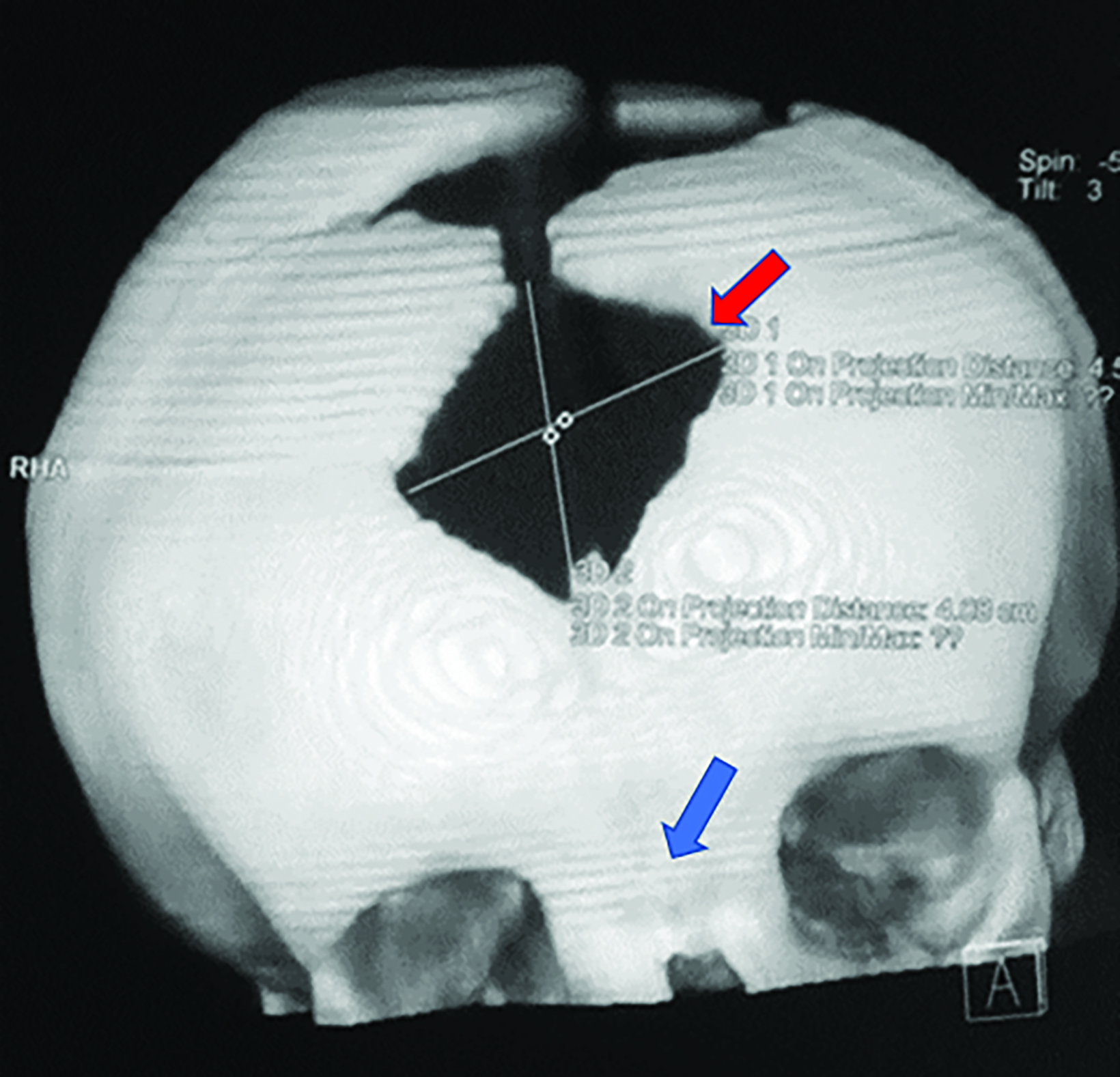
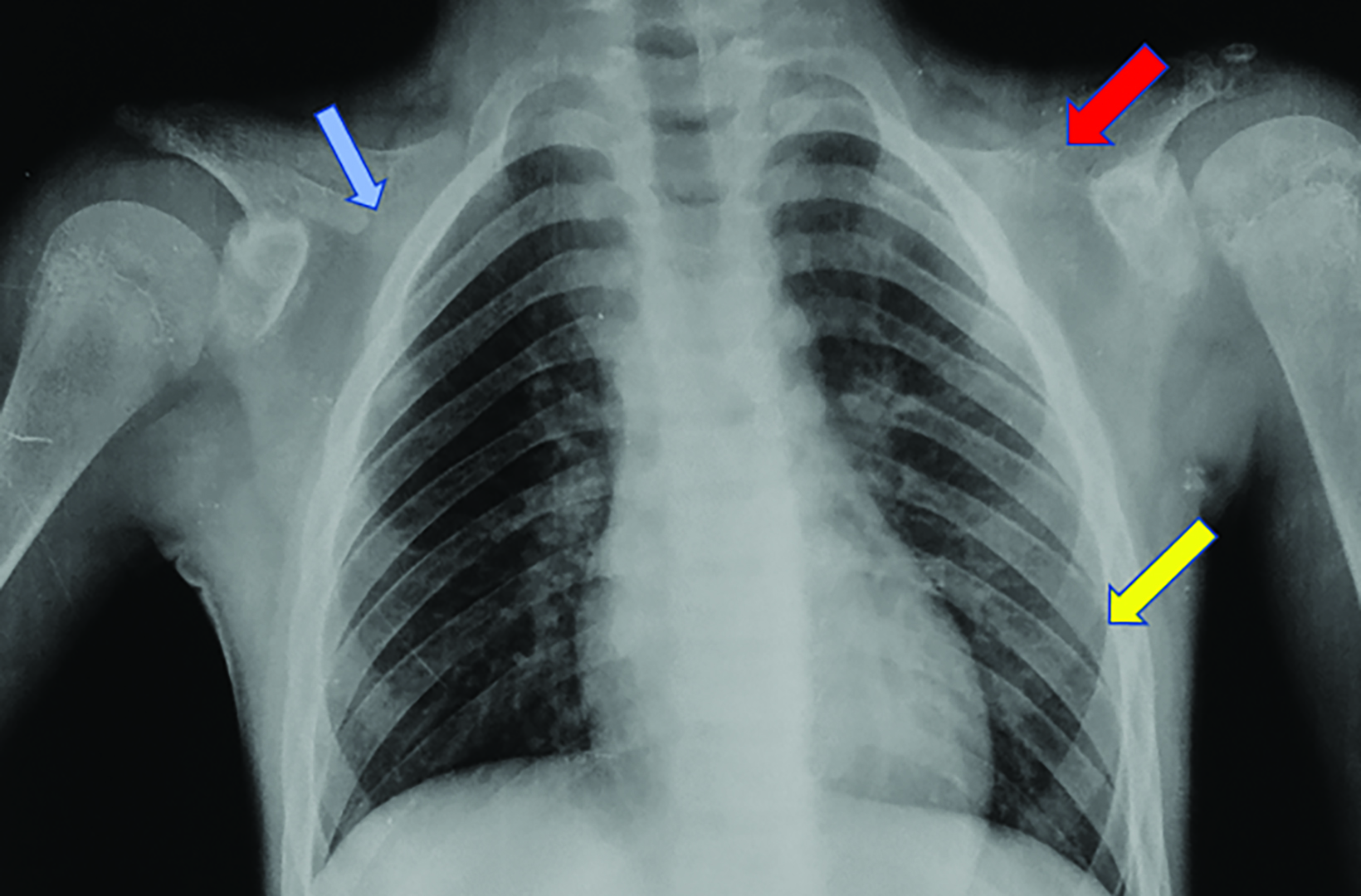
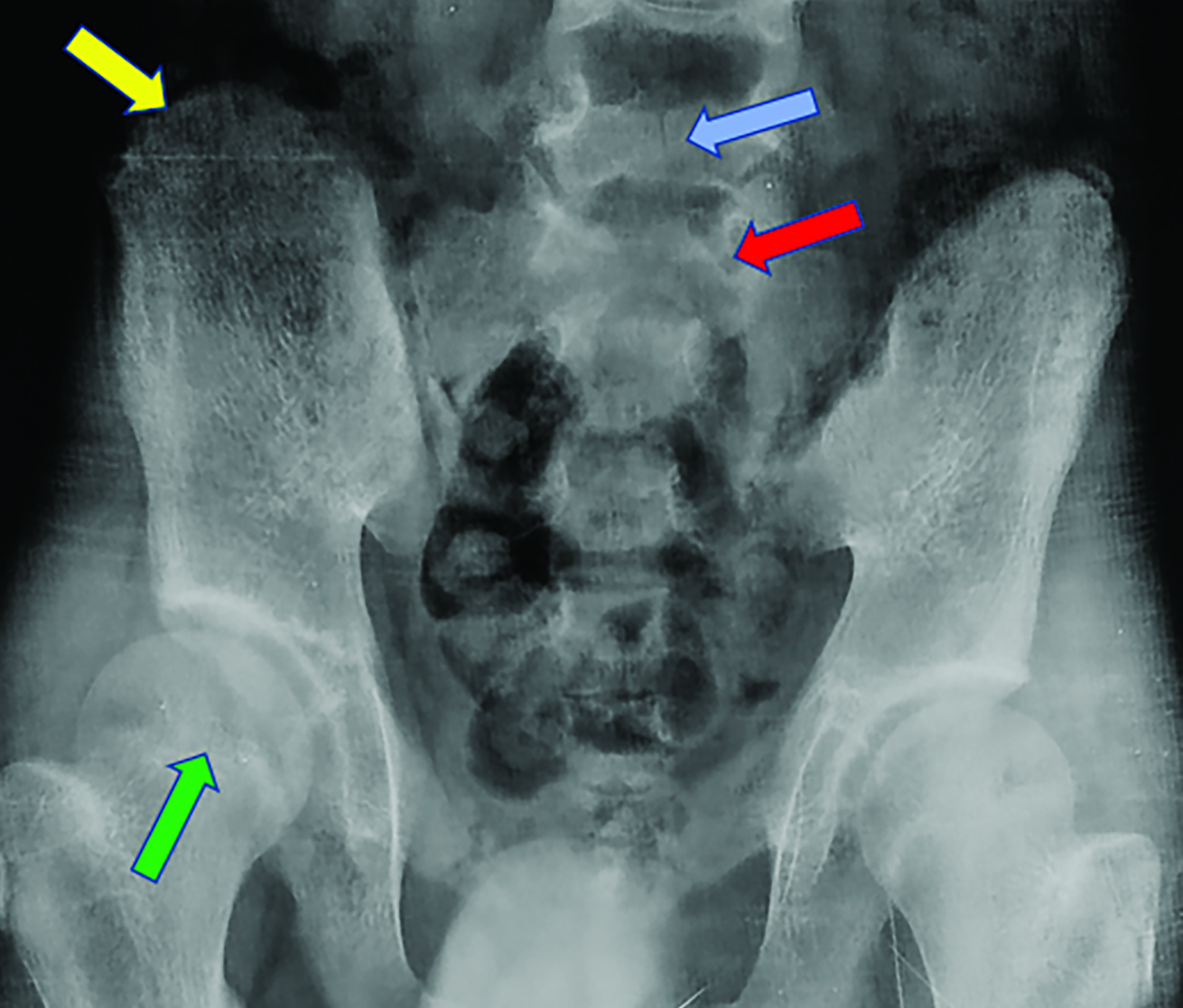
Nonenhanced computed tomography (CT) head with 3D reconstruction and a radiographic skeletal survey were performed. 3D surface rendering of the skull showed open fontanelles, and wide metopic and sagittal sutures with Wormian bones (Figures 1, 2). Chest radiography showed a narrow, bell-shaped thorax, wide and oblique ribs, and a hypoplastic medial clavicle on the right and an absent clavicle on the left (Figure 3). Pelvic radiography showed spina bifida at the fifth lumbar and first sacral vertebrae, narrow iliac flanks, and bulky femoral heads (Figure 4). Foot radiography showed short and tapered distal phalanges, 5th-digit clinodactyly, and short 4th metatarsals (Figure 5).
Diagnosis
Cleidocranial dysplasia
Discussion
Cleidocranial dysplasia is disorder affecting the teeth, bones, and cartilage, occurring with a frequency of 1:1 million. The underlying cause is a mutated RUNX2 gene located on the short arm of chromosome 6, which may be inherited in an autosomal dominant pattern or result from a new mutation.1
The usual clinical presentation is dwarfism and dental and skeletal deformities. Osteoporosis and a predisposition to ear and sinus infections are also common. Cognition is preserved.2
Imaging is needed to confirm the diagnosis, rule out similar conditions, and plan surgical management. Key diagnostic features are absent or hypoplastic clavicles, brachycephaly, and open fontanelle(s). Other skull findings include the presence of Wormian bones within the widened cranial sutures, a hypoplastic sphenoid body, frontal and parietal bossing, and basilar invagination.
Other chest findings include small scapulae and glenoid fossae, narrow and downward-sloping thorax, and rib deformities. In the axial skeleton, spina bifida or delayed vertebral and pelvic maturation may be observed. In the extremities, coxa vara, genu valgum, coned epiphyses, tapered phalanges, elongated 2nd and 5th metacarpals, or additional ossification centers at the bases of the metacarpals may be observed. Supernumerary teeth can be observed on orthopantomogram and CT.2,3
Clinical examination and skeletal survey radiographic evaluation are often adequate for diagnosis. Genetic testing for the RUNX2 gene can be considered in the setting of an atypical physical examination and skeletal survey. Fetal sonography can be useful in diagnosing this condition in utero.2
Management includes surgical correction of skeletal and dental deformities.4,5 The use of protective gear such as a helmet is advised to prevent head trauma in high-risk activities. Prevention of osteoporosis and infection in the ears and sinuses are important. Genetic counseling should be offered to persons with a family history if they are planning to have a child. Affected females need close surveillance during pregnancy, as the rate of cephalopelvic disproportion is high.2
Awareness of radiographic features is also important to help differentiate cleidocranial dysplasia from similar entities. The primary differential consideration is pyknodysostosis, in which skull changes and the absence of the clavicles are also seen. Key differentiating features of pyknodysostosis are increased bone density and an obtuse mandible.3,6 Other differential diagnoses include acro-osteolysis, which is characterized by tapering of the digits resulting from phalangeal resorption; mandibuloacral dysplasia, in which a hypoplastic mandible is seen without small clavicles and tapering digits; hypothyroidism and hypophosphatasia, in which Wormian bones may be seen; and Crane-Heise syndrome, characterized by cleft palate, craniofacial dysmorphism, and absent clavicles.2,3
Conclusion
Cleidocranial dysplasia is an autosomal-dominant disorder with variable expression. Knowledge of its radiological appearance is important for correct diagnosis, monitoring, and preventive treatment of primary and secondary complications.
References
- Otto F, Kanegane H, Mundlos S. Mutations in the RUNX2 gene in patients with cleidocranial dysplasia. Hum Mutat. 2002;19(3):209–216. doi:10.1002/humu.10043.
- Machol K, Mendoza-Londono R, Lee B. Cleidocranial dysplasia spectrum disorder. 2006 Jan 3 [Updated 2017 Nov 16]. In: Adam MP, Ardinger HH, Pagon RA, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2020. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1513/
- Renton P, Green R. Congenital skeletal anomalies: skeletal dysplasias, chromosomal disorders. 2003. In: Sutton D, editor. Textbook of Radiology and Imaging (restricted south Asia edition) Vol.2. 7th ed. India: Churchill Livingstone. 1107-1152.
- Balioğlu MB, Kargın D, Albayrak A, Atıcı Y. The treatment of cleidocranial dysostosis (Scheuthauer-Marie-Sainton syndrome), a rare form of skeletal dysplasia, accompanied by spinal deformities: a review of the literature and two case reports. Case Rep Orthop. Volume 2018 |Article ID 4635761 | 10 pages | https://doi. org/10.1155/2018/4635761.
- Park TK, Vargervik K, Oberoi S. Orthodontic and surgical management of cleidocranial dysplasia. Korean J Orthod. 2013; 43(5):248–260. doi:10.4041/ kjod.2013.43.5.248.
- Ramaiah KK, George GB, Padiyath S, Sethuraman R, Cherian B. Pyknodysostosis: report of a rare case with review of literature. Imaging Sci Dent. 2011;41(4): 177–181. Doi:10.5624/isd.2011.41.4.177.
Citation
R BNR. Cleidocranial Dysplasia. Appl Radiol. 2022;(6):40-42.
November 2, 2022