Complete gastric outlet obstruction secondary to oligocystic pancreatic serous cystadenoma
By Zarour CC, Vellanki S, Sekhon J, Mian A, Gerasymchuk G


CASE SUMMARY
A 90-year-old female presented with nausea and vomiting. The patient reported a decrease in appetite and fluid intake for 3 weeks. Upon physical examination, the patient’s abdomen was distended and tender to palpation in the epigastric region. Decreased bowel sounds were also noted. A nasogastric tube was placed for suction decompression. A CT abdomen with oral and intravenous contrast was performed, demonstrating gastric distention with mechanical obstruction by multiple cystic lesions consistent with oligocystic pancreatic serous cystadenoma. An esophagogastroduodenoscopy was performed, and confirmed complete gastric outlet obstruction occurring at the duodenal bulb. The patient underwent a gastrojejunostomy.
IMAGING FINDINGS
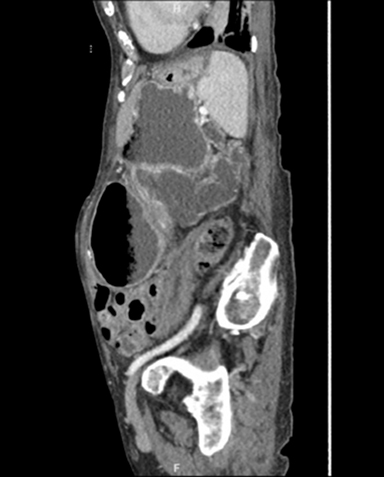
Contrast CT of the abdomen demonstrated gallbladder distention, common bile duct dilatation up to 1.4 cm, and massive gastric distension measuring up to 22 cm in the AP dimension. The pancreatic head and uncinate process were intact, while the body and tail were replaced with multiple variously sized cystic lesions (Figure 1).
DIAGNOSIS
Complete gastric outlet obstruction secondary to oligocystic pancreatic serous cystadenoma
DISCUSSION
Pancreatic Serous Cystadenoma (PSC) is a benign pancreatic neoplasm that occurs in the 5th to 7th decade of life, and is more common in females than in males with chronic pancreatitis. There are two different types of PSC; the more common microcystic, and the less common macrocystic, or oligocystic, PSC.1 Most patients diagnosed with PSC tend to be asymptomatic if the lesion is less than 4 cm. However, lesions larger than 4 cm can produce symptoms ranging from mass effect, such as abdominal discomfort, to multiple episodes of vomiting due gastric outlet obstruction.1
Diagnosis consists of MRI or CT imaging. In this case, CT was the preferred method due to the concerns of possible obstruction. For further characterization of the cystadenomas, cross-sectional imaging helped determine cyst features and malignant patterns.2 PSC presents as a well-demarcated multicystic lesion with central scarring visible in fewer than 20% of cases.3 Oligocystic PSC measuring greater than 5 mm have a lobulated appearance. Septations may or may not be present.4 Endoscopic ultrasound with fine-needle aspiration provides a high- quality image of the pancreas and allows for lesion sampling.5
After diagnosis, further management depends on cystic size and symptoms. Cysts measuring less than 4 cm or which have benign characteristics, warrant surveillance imaging with no intervention. Only symptomatic cysts measuring 5 cm require surgical intervention to relieve ongoing symptoms.5 Surgical removal of the PSC is curative, with an extremely low recurrence rate.6
CONCLUSION
Pancreatic serous cystadenomas are grouped into either microcystic or oligocystic (macrocystic). Oligocystic pancreatic serous cystadenomas account for fewer than 10% of all cases. Nonetheless, they are a complication of chronic pancreatitis. When symptoms of complete gastric outlet obstruction occur, further investigation with CT imaging or MRI is required. Variables including size, location, and symptom severity, allow for surgical intervention as a treatment option. Gastrojejunostomy was successful in this patient, with no further complications.
REFERENCES
- Tseng JF, Warshaw AL, Sahani DV, et al. Serous cystadenoma of the pancreas: tumor growth rates and recommendations for treatment. Ann Surg. 2005; 242:413.
- King JC, Ng TT, White SC, et al. Pancreatic serous cystadenocarcinoma: a case report and review of the literature. J Gastrointest Surg. 2009; 13:1864-1868.
- Centeno BA, Lewandrowski KB, Warshaw AL, et al. Cyst fluid cytologic analysis in the differential diagnosis of pancreatic cystic lesions. Am J Clin Pathol. 1994;101:483.
- Vege SS, Ziring B, Jain R, et al. American gastroenterological association institute guideline on the diagnosis and management of asymptomatic neoplastic pancreatic cysts. Gastroenterology. 2015; 148:819.
- Al-Haddad M, Gill KR, Raimondo M, et al. Safety and efficacy of cytology brushings versus standard fine-needle aspiration in evaluating cystic pancreatic lesions: a controlled study. Endoscopy. 2010; 42:127.
- Genevieve L. Bennett et.al, Radiologic-Pathologic Conferences of the Massachusetts General Hospital Serous Cystadenoma of the Pancreas, AJR 1993;161:786.
Prepared while Dr. Zarour was practicing as a Diagnostic Radiology Resident; Dr. Vallenki was practicing as an Internal Medicine Resident; and Dr. Gerasymchuk was practicing as a Board Certified Radiologist, all at St. Joseph Mercy Oakland Hospital, Pontiac, MI. Sekhon, an MS4 at Ross University, and Mian, an MS3 at Windsor University School of Medicine, were completing their clinicalclerkships at St. Joseph Mercy Oakland Hospital, Pontiac, MI.