Intraosseous Lipoma of the Sacrum
By Patterson SP, Patterson D, Walker SM
CASE SUMMARY
A 29-year-old presented two months postpartum with persistent low back pain and coccydynia. Obstetrical history revealed a normal spontaneous vaginal delivery. After delivery, she reported significant pain in her tailbone. Initially the pain abated with non-steroidal anti-inflammatory therapy; however, the coccydynia worsened over the next month with increased difficulty sitting to the point where breastfeeding was possible only in a standing position. Because of the persistent pain, the patient was referred for orthopedic consultation. Initial imaging workup included radiography and MRI.
IMAGING FINDINGS
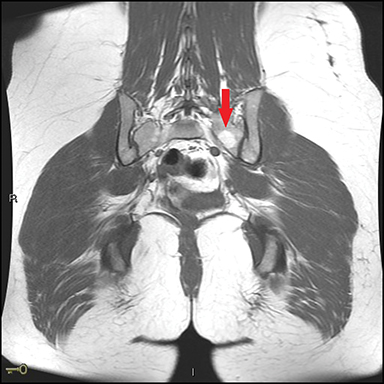
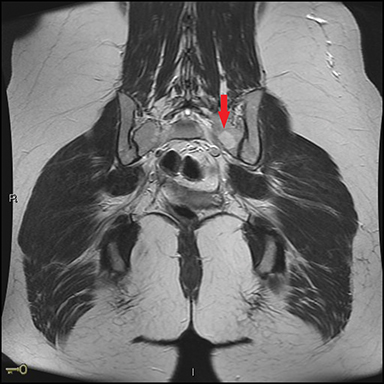
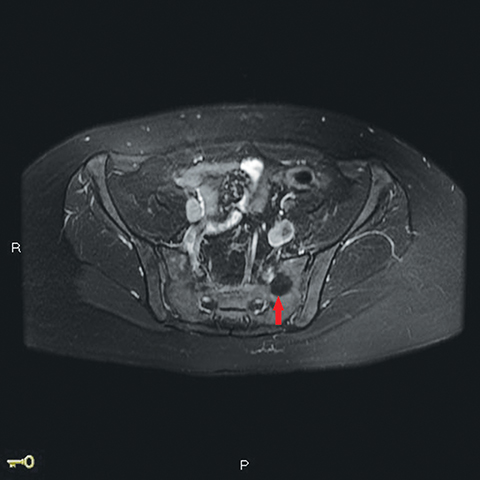
Pelvic radiographs were unrevealing, with no osseous or articular abnormalities. Subsequent pelvis MRI revealed intact muscles, ligaments, and tendons. The coccyx and sacroiliac joints appeared normal. In the left inferior sacrum, a 1.7 cm well-circumscribed lesion was hyperintense on T1 and T2 (Figure 1). The lesion had a narrow zone of transition and demonstrated signal dropout on fat-suppressed sequences (Figure 2). It had no associated aggressive features such as surrounding edema or soft tissue invasion.
DIAGNOSIS
Intraosseous lipoma of the sacrum
DISCUSSION
Intraosseous lipomas are rare, accounting for 0.1% to 2.5% of primary bone tumors.1 No age or sex predilection has been reported. These tumors are often asymptomatic and generally are discovered incidentally. Symptomatic intraosseous lipomas typically present with pain, local swelling, or tenderness.1,2 The metaphysis of long bones and the calcaneus are the most common locations. Pelvic involvement is uncommon; only 4 cases of sacral lipoma have been reported in the literature to the best of our knowledge.3,4,5,6
Lipomas are benign with little potential for malignant transformation; familiarity with the imaging characteristics avoids unnecessary work-up and potential biopsy. Intraosseous lipomas that do not affect bone stability may be treated conservatively and require no follow-up.3 Cases with imminent fractures are treated with curettage and bone grafting.7
As in our case, radiographs are often falsely negative. If visible on radiographs, intraosseous lipomas are usually well-defined, lucent lesions without aggressive features.2,8 On CT they typically appear as well-defined lytic lesions with a thin, sclerotic rim and with Hounsfield units of fat density.3,8 Intraosseous lipomas are hyperintense on T1 and T2 MR sequences.2,9 Fat-suppressed images demonstrate signal dropout; the lesions are isointense to adipose tissue.9
Milgram1,7,8,9 outlined a 3-stage classification for intraosseous lipomas combining both histological and radiologic features: 1) Uniformly adipose tumors of viable fat cells; 2) A mixture of viable fat cells, fat necrosis, and calcifications; and 3) Necrotic fat, cystic formation, and reactive woven bone.
In this case, the MR images demonstrated uniformity of fat-signal intensity throughout the lesion, consistent with a Stage 1 lipoma. After reviewing the patient’s symptoms and consulting with the orthopedic surgeon, we believed the lesion to be incidental with no further imaging or histopathologic correlation required. The patient returned in 1 month and reported an improvement of symptoms with conservative management as well as a return to normal daily activities.
CONCLUSION
Our case illustrates several points. First, the discovery of incidental findings, including benign bone tumors, has markedly increased with increased utilization of cross-sectional imaging. Second, while rare, intraosseous lipomas are an important consideration in the differential diagnosis of osseous lesions, particularly when asymptomatic and incidentally discovered. Third, familiarity with the imaging characteristics of these “don’t touch” lesions helps avoid unnecessary imaging workup and biopsy.10
REFERENCES
- Yazdi HR, Radouli B, Borhani A, Noorolahli MM. Intraosseous Lipoma of the Femur: Image Findings. J Ortho Case Reports. 2014; 4(1) 35-38.
- Mohapatra NC, Sahoo A, Mishra J, Kumar HV. Intraosseous Lipoma of the Ilium: A rare case report with review of literature. Oncol J India. 2017; 1: 10-12.
- Campbell RS, Grainger AJ, Mangham DC et al. Intraosseous lipoma: report of 35 new cases and a review of the literature. Skeletal Radiol. 2003; 32(4): 209-222.
- Milgram JW. Involuted intraosseous lipoma of sacrum. Spine. 1991; 16: 243–245.
- Ehara S, Kattapuran SV, Rosenberg AE. Case report 619. Intraosseous lipoma of the sacrum. Skeletal Radiol. 1990;19: 375–376.
- Kamekura S, Nakamura K, Oda H, Inokuchi K, Iijima T, Ishida T. Involuted intraosseous lipoma of the sacrum showing high signal intensity on T1-weighted magnetic resonance imaging (MRI). J Orthop Sci. 2002; 7:274–280.
- Bagatur AE, Raleinkaya M, Dogan A, Gur S, Mumeoglu E, Albayrak M, et al. Surgery is not always necessary in intraosseous lipoma. Orthopedics 2010; 33:306.
- Mannem RR, Mautz AP, Baynes KE, Zambrano EV King DM. AIRP Best Cases in Radiologic-Pathologic Correlation. RadioGraphics. 2012; 32: 1523-1528.
- Blackshin MF Ende N, Bnevenia. Magnetic resonance imaging of intraosseous lipomas: radiologic-pathologic correlation. Skeletal Radiol. 1995; 24: 37-41.
- Helm C. 2014. Chapter 4 in Fundamentals in Skeletal Radiology. 4th ed. Philadelpha (PA): Saunders.
Affiliations: St. Clair Hospital, Pittsburgh, PA (Drs Scott Patterson and Walker); Children’s Hospital, Pittsburgh, PA (Dr Dina Patterson).