Radial scar associated with calcium oxalate crystals

Click here to view and interact with the DICOM images for Figure 2 in the Exa-PACS zero foot print viewer provided by Viztek.
Case Summary
A 55-year-old female with history of HIV and Hepatitis C presents for annual screening mammogram where a 2 cm area of architectural distortion is identified in the right lower outer breast seen only on the DBT images. Additional mammographic diagnostic imaging confirmed the area of architectural distortion. On US, the patient had no sonographic correlate for the DBT finding. Thus, the patient had a stereotactic biopsy of the architectural distortion with pathology consistent with radial scar.
Imaging Summary
Click here to view and interact with the DICOM images for Figure 2 in the Exa-PACS zero foot print viewer provided by Viztek.
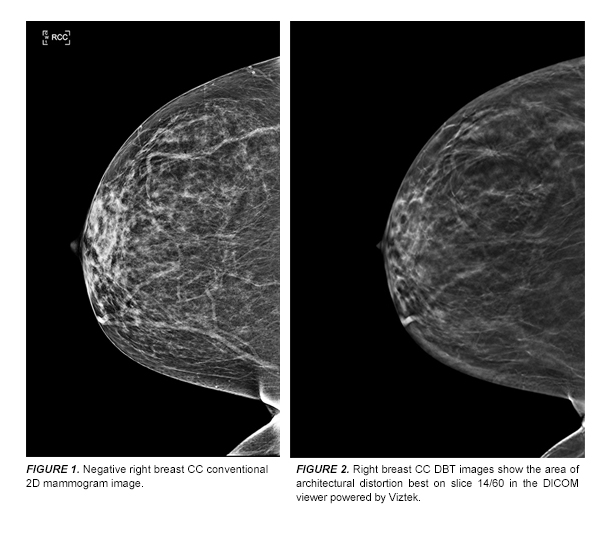
The right breast CC 2D digital mammogram (Figure 1) was read as benign.
Selected right breast CC images from DBT show that the area of architectural distortion is in the right outer breast middle depth (best seen on Right CC slice 14/60).
Discussion
The cause of a radial scar is unclear. There is a slightly increased risk of subsequent development of carcinoma when radial scar is found.1,3 In women older than 50 years, there is an increased frequency of carcinoma and atypical hyperplasia associated with larger radial scars.2 Currently, most authorities agree that if a radial scar is identified on core-needle biopsy, it should be surgically excised.4
DBT better evaluates masses, architectural distortion, and asymmetries compared with conventional 2D digital mammography because superimposed tissue that confounds the clear depiction of a lesion on 2D digital mammography is out of the plane of focus with DBT.5 This allows the radiologist to be more accurate in describing the findings and more sensitive in detecting smaller lesions previously obscured by dense breast tissues.5 When compared with digital mammography alone, Skaane et al. found the combination of DBT and digital mammography resulted in a statistically significant 27% increase in cancer detection rate and a statistically significant reduction in false-positive findings by 15%.6 Skaane et al. also found that compared to mammography alone, the combination of mammography with DBT resulted in a statistically significant 40% higher detection rate for invasive cancers.6
Conclusion
DBT offers an advantage for evaluation of masses, architectural distortion, and asymmetries compared with conventional 2D digital mammography because superimposed tissue that confounds the clear depiction of a lesion on 2D digital mammography is out of the plane of focus with DBT.5 When compared with digital mammography alone, the combination of DBT and digital mammography has shown to increase cancer detection rate and decrease the number of false-positives.6
References:
- Kopans DB.Breast Imaging, 3rd edition. Lippincott, Williams, and Wilkens, 2006.
- Sloane JP, Mayers MM. Carcinoma and atypical hyperplasia in radial scars and complex scloerosing lesions: importance of lesion size and patient age.Histopathology. 1993; Sep;23(2):225-31.
- Jacobs TW, Byrne C, Colditz G, et al.Radial scars in benign breast-biopsy specimens and the risk of breast cancer. N Engl J Med. 1999;Feb11;340(6):430-6.
- Schnitt, SJ & Collins LC. Biopsy Interpretation of the Breast. Lippincott, Williams, and Wilkens, 2008.
- Zuley ML, Bandos AI, Ganott MA, et al.Digital Breast Tomosynthesis versus Supplemental Diagnostic Mammographic Views for Evaluation of Noncalcified Breast Lesions. Radiology. 2013;266(1):89–95.
- Skaane P, Bandos AI, Gullien R, et al. Comparison of Digital Mammography Alone and Digital Mammography Plus Tomosynthesis in a Population-based Screening Program.Radiology. 2013;267:1:47-56.