Recurrent lymphoma in the left acetabulum
Supplement to Applied Radiology December 2012, sponsored by Philips
Dr. Muzaffar is a Fellow and Dr. Osman is the Program Director of the Division of Nuclear Medicine, Department of Radiology, Saint Louis University Hospital, St. Louis, MO.
Case summary
A 75-year-old female presented to our outpatient clinic for her annual follow-up for lymphoma. She had been diagnosed 5 years prior with marginal zone lymphoma in the mediastinum with recurrent pleural-effusions status post-chemotherapy and eventually pleurodesis. Since that time, she had multiple negative positron emission tomography and computed tomography (PET/CT) scans.
Imaging findings
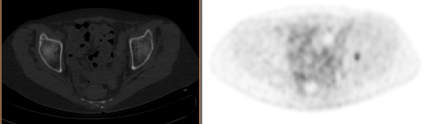
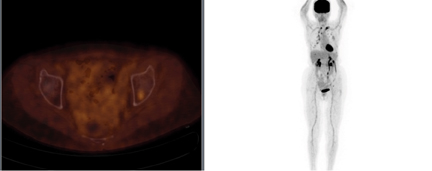
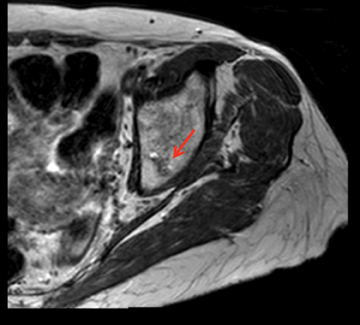
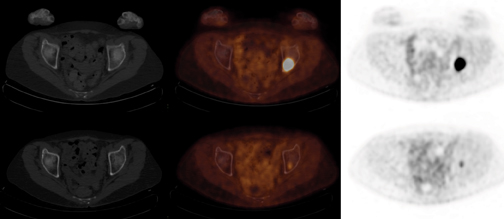
PET/CT demonstrated stable focal uptake in the thyroid and post-pleurodesis changes in the chest (Figure 1). A new subtle 18F-fluorodeoxyglucose (18F-FDG) focus was present in the left acetabulum with normal CT raising the suspicion for metastasis (Figure 1). Magnetic resonance imaging (MRI) demonstrated an irregular lesion within the left acetabulum with increased signal on short T1-inversion recovery (STIR) and low signal on T1 and T2, suggestive of an intraosseous vascular lesion (Figure 2). The follow-up PET/CT demonstrated significant increased size and FDG uptake in the acetabular lesion consistent with disease progression (Figure 3).
Diagnosis
Recurrent lymphoma in the left acetabulum
Discussion
Lymphoma is a malignancy of lymphocytes and is usually present as a solid tumor composed of lymphoid cells. Lymphoma can be classified into 2 groups, Hodgkin lymphoma and non-Hodgkin lymphoma (NHL). Hodgkin lymphoma derives from abnormal B cells whereas NHL can arise from abnormal B or T cells. The malignant cells accumulate in lymph nodes, but can also involve other organs, such as skin, brain, bowel, and bones. Since these lymph nodes or extranodal sites are typically subtle, they are often felt to be normal or reactive on CT. However, 18F-FDG PET/CT helps differentiate the indeterminate cases. A recent study found 18F-FDG PET/CT was more accurate than CT alone in early detection of bone metastasis and improved staging in 15% of the study population.1
The use of 18F-FDG PET/CT has been gaining momentum in diagnosing, staging, and restaging many cancers and is often better than anatomical imaging alone.2 According to the Academy of Molecular Imaging, there are more than 5,000 PET/CT systems installed worldwide, making it one of the fastest growing imaging modalities.3 The National Oncologic PET Registry (NOPR) was developed in 2006 to collect data on the clinical utility of PET. As of June 2012, it has evaluated over 280,000 PET studies performed at 1,756 centers.4 The fusion of functional and anatomic imaging continues to evolve and provide valuable clinical information. PET/CT provides additional information as compared to either modality alone and has become the first-line imaging modality for tumor staging, restaging, and therapy response in various types of cancer.5
Another advancement of PET/CT is the use of time-of-flight (TOF) to improve lesion detection, especially in heavier patients. Conventional PET scanners detect gamma rays from radioisotopes injected in the body. However, they do not account for the time it takes to reach the detector. TOF will account for this time, resulting in an enhanced signal-to-noise ratio. TOF PET has been shown to significantly improve lesion detection compared to non-TOF images of 8.3% in the liver and 15.1% in the lungs. The greatest improvement was for lower lesion contrasts.6 The availability of such technology improves our ability to characterize lesions and affect treatment decisions and patient management.
Conclusion
A bone biopsy was performed and revealed metastatic lymphoma. The patient was treated with chemotherapy and is now in remission. PET/ CT images can be used in the evaluation, diagnosis, and staging of cancer. As in this case, PET/CT was both more sensitive and specific than MRI.
References
- Evangelista L, Panunzio A, Polverosi R, et al. Early bone marrow metastasis detection: The additional value of FDG-PET/CT vs. CT imaging. Biomed Pharmacother. 2012. 66:448
- Czernin J, Allen-Auerback M, Schelbert HR. Improvements in cancer staging with PET/CT: Literature-based evidence as of September 2006. J Nucl Med. 2007;48(Supplement 1):78S-88S.
- “International Survey of PET/CT Operations and Oncology Imaging 2010.” Academy of Molecular Imaging. http://www.ami-maging.org/index.php?option=com_ content&task=view&id=181. Accessed September 19, 2012.
- “NOPR Update: Monthly Status Report.” National Oncologic PET Registry. http://www.cancerpetregistry.org/status.htm. Accessed September 19, 2012.
- Antoch G, Vogt FM, Freudenberg LS, et al. Whole-body dual modality PET/CT and whole-body MRI for tumor staging in oncology. JAMA. 2003;2900:3199-3206.
- El Fakhri G, Surti S, Trott CM, et al. Improvement in lesion detection with whole-body oncologic time-of-flight PET.J Nucl Med. 2011;52:347-353.