Septate uterus
Images

Septate uterus
Findings
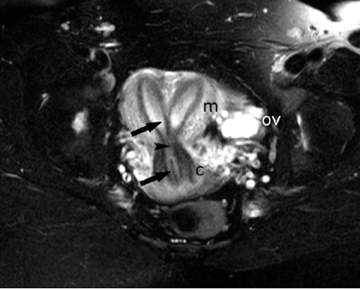
Two endometrial cavities with normal external contour of the uterine fundus. Uterine septum extends through cervix.
Discussion
Müllerian duct anomalies in women include lack of development (hypoplasia, aplasia, or unicornuate uterus), lack of midline fusion (didelphys or bicornuate uterus), and incomplete resorption of midline tissue during fusion (septate and arcuate uteri). The noncomplex anomalies which can show 2 symmetric endometrial cavities are septate, bicornuate, and didelphys uteri. Distinction between a septate uterus and either the didelphys or bicornuate uterus is important if infertility warrants surgical repair.
Because the endometrial cavities in the didelphys or bicornuate uteri are separated by normal myometrium, a pregnancy will normally implant and be more likely to proceed. Surgery is thus rarely performed and would entail metroplasty via a laparotomy. The septum in a septate uterus has abnormal vascularization and mechanics. Implantation on the septum results in frequent spontaneous first-trimester pregnancy loss. The septum is therefore removed; this can be done using a simpler hysteroscopic approach. Distinguishing a didelphys or bicornuate uterus from a septate uterus is critical.
Embryologically, 2 processes occur during Müllerian development, lateral fusion and segmental resorption. The paired Müllerian ducts undergo lateral fusion to form the uterus, cervix, and upper vagina. Uterine didelphys is complete uterine nonfusion with 2 uteri and 2 cervices separated by a normal myometrium. In a bicornuate uterus, a normal muscular septum can extend to the internal os (partial or bicornuate unicollis) or close to the external os (complete or bicornuate bicollis).
Both the didelphys and bicornuate have a deep fundal indentation (>1 cm) between 2 symmetric horns containing endometrium. A didelphys and bicornuate uterus represent a continuum of fusion. A didelphys and an extreme bicornuate uterus with near complete lack of fusion may be difficult to distinguish, but is of low importance clinically. A septate uterus has undergone complete fusion. The external contour of the uterus is therefore normal (Figure 1).
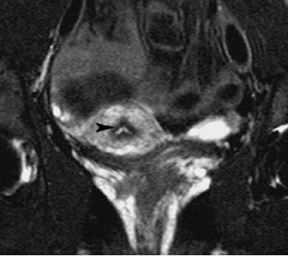
As lateral fusion is occurring, septal resorption is also occurring. The intervening midline vertical septum between the uterus, cervix, and upper vagina is resorbed segmentally beginning in the lower uterine segment and progressing in both directions,1 as the current case illustrates (Figure 1 and 2). The septum tends to be mainly muscular superiorly (although histologically different from normal myometrium) and more fibrous and thinner towards the cervix.
Septal resorption may be arrested at any point, resulting in variable lengths of septum in the septate uterus2 and infrequently in the bicornuate uterus. The myometrium in a partial bicornuate uterus may extend to the lower uterine segment with communication between the 2 cavities at that level (and thus defining it as a bicornuate uterus). However, an apparent “duplicated” cervix can result from a nonresorbed fibrous septum in the cervix.3
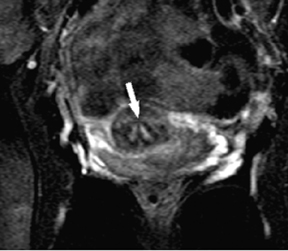
All entities may independently have a duplicated upper vagina.1 Upper vaginal duplication is present in 75% of didelphys uterus, but occurs in 25% of the bicornuate and septate uteri in 25% (Figure 3) and rarely with a normal uterus.
Because of the variable presence of a uterine and cervical septum and a duplicated upper vagina in didelphys, bicornuate, and septate uteri, the presence or absence of cervical or upper vaginal duplication are not reliable in distinguishing between them. A septate uterus with a complete septum and duplicated upper vagina is not infrequently misdiagnosed as a didelphys uterus. Tissue characterization by MRI is also not reliable given that the septum in the uterine body in all entities is predominantly myometrial tissue.
Conclusion
Making the correct diagnosis is best made by first evaluating the external contour of the uterus. A normal contour excludes a didelphys or bicornuate and the uterus is either normal or septate. With the correct anomaly now established, the presence and extent of a uterine septum and upper vaginal duplication is independently evaluated.
These symmetric Müllerian anomalies should be differentiated from the unicornate uteri variations and the infrequent complex anomalies. A unicornuate uterus with a communicating rudimentary horn have asymmetrically sized horns unlike a bicornuate uterus. A didelphys uterus with obstructed hemivagina is recognized from the simple didelphys given its constellation of anomalies.
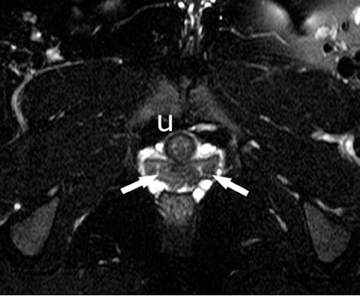
MRI is the most accurate modality in characterizing the type of abnormality and is used when other imaging studies are inconclusive. A T2-weighted acquisition in the coronal oblique plane, parallel to the long axis of the uterus, best shows the external contour. This case of a septate uterus shows a normal sized uterus with a normal external contour and a duplicated vagina. A midline septum separates 2 endometrial canals and cervices. Some resorption had occurred at the isthmus, allowing some communication between the lower endometrial canals.
- Troiano RN, McCarthy SM. Müllerian duct anomalies: Imaging and clinical issues. Radiology. 2004;233:19-34.
- Chang AS, Siegel CL, Moley KH, et al. Septate uterus with cervical duplication and longitudinal vaginal septum: A report of five new cases. Fertil Steril. 2004;81:1133-1136.
- La Fianza A, Campani R, Villa A, et al. Communicating bicornuate uterus with double cervix and septate vagina: An uncommon malformation diagnosed with MR imaging. Eur Radiol. 1997;7: 235-237.