Stress Fracture
By Holl N, Thierfelder KM, Ellenrieder M, Mittelmeier W, Weber M


Case Summary
A young adult presented with a three-month history of persistent pain in the right thigh after running a marathon. A seasoned amateur longdistance runner, the patient endorsed a rigorous training protocol. The patient’s pain was increased during hip extension exercises. Physical examination revealed free range of motion (ROM) of both hips and knee joints. Nonspecific pain in the right thigh could be provoked by forced passive ROM testing of the hip. No localized tenderness or swelling were evident. Lumbar spine and sacroiliac joints were clinically normal.
Imaging Findings
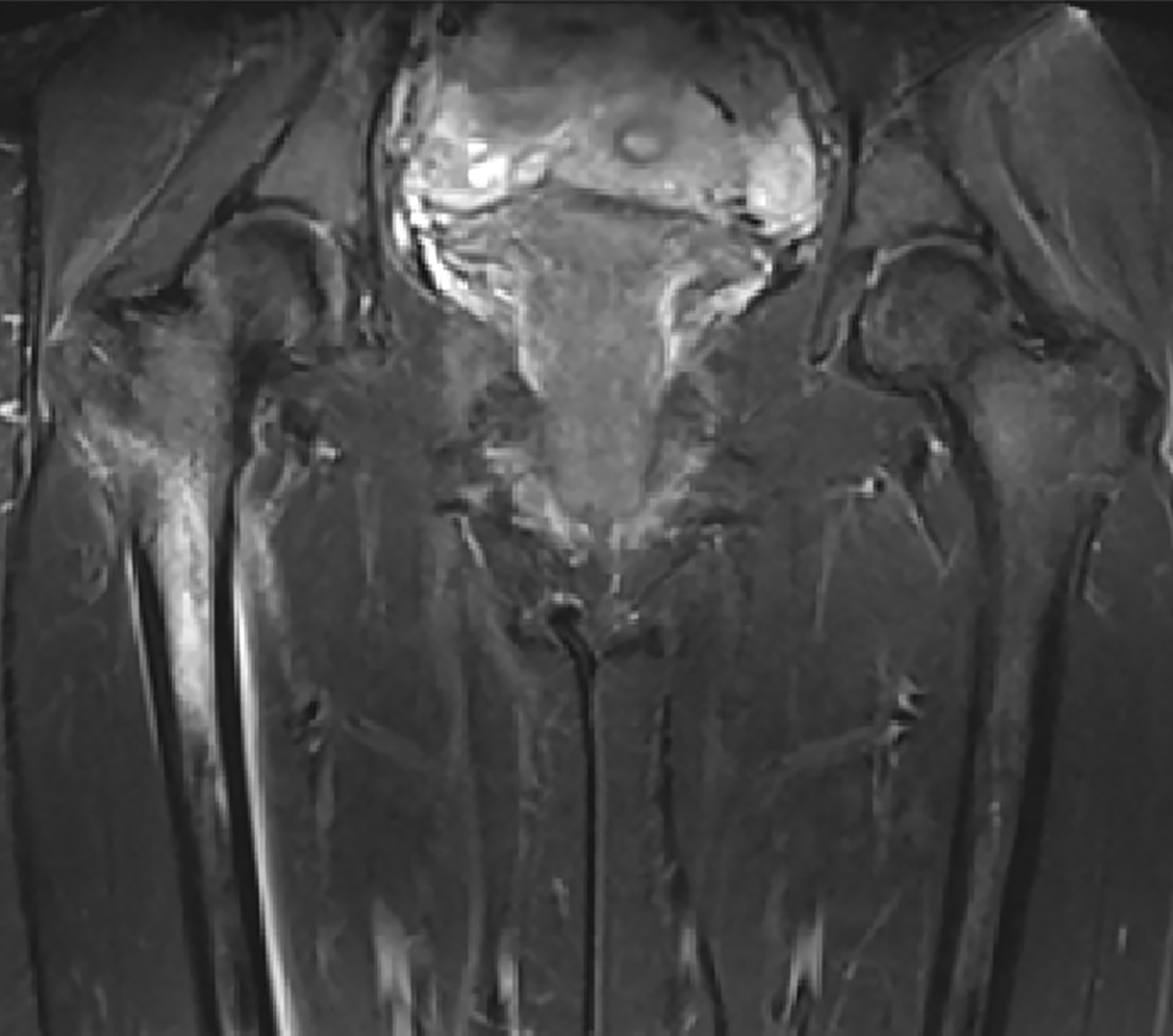
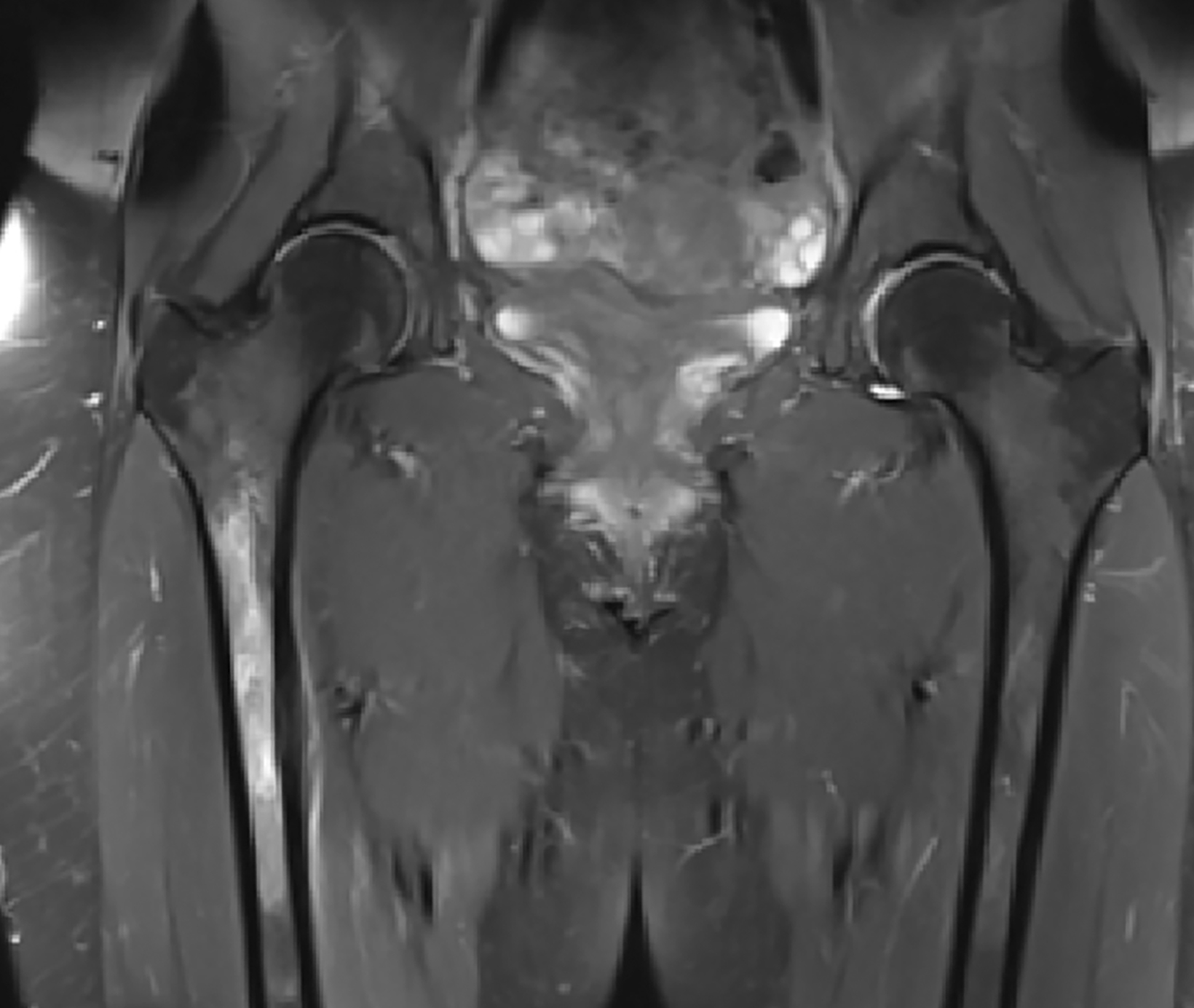
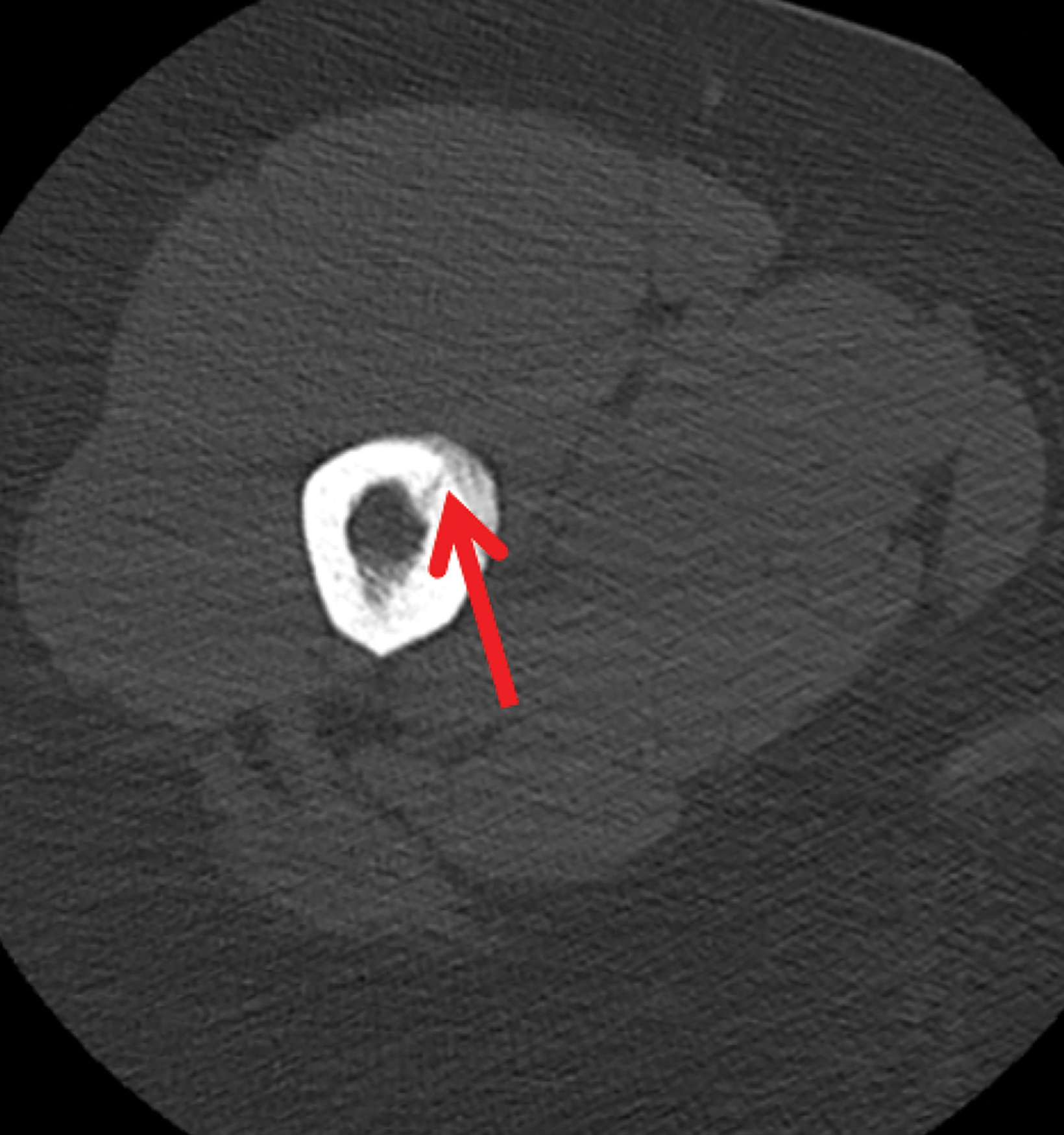
Findings on radiographs were unremarkable. Magnetic resonance imaging (MRI) revealed intraosseus signal changes on T1 and T2-TIRM sequences in the proximal femoral diaphysis (Figure 1) representing bone marrow edema. Initial, conservative therapy consisted of six weeks of partial weight-bearing. Follow-up MRI six weeks post-treatment demonstrated persistent bone marrow edema, as did a third MRI examination eight weeks after initial imaging. A noncontrast computed tomography scan three months after presentation revealed a non-displaced fracture of the right femoral diaphysis extending from middle of the shaft up to the neck (Figure 2) with callus formation around the shaft
Diagnosis
Stress fracture
Discussion
Femoral fractures are among the most common sites of stress-related injuries. This is partially explained by the fact that the largest bending moments during movements occur at the proximal femur.1 In locomotor tasks, such as running, the impact phase constitutes peak magnitudes of force. The characteristics of the loading stimulus (eg, frequency of loading, number of load repetitions) are essential for injury development.2 An accumulation of structural damage could result in complete fracture. Kang, et al,3 retrospectively reported on seven cases of femoral stress fractures in female athletes. Sudden and abrupt changes in the athletes’ training regimen were identified as the main factors in the development of stress fractures. In contrast, in the case presented here, an abrupt change in training intensity could not be identified. A three- to four-month preparation period for a marathon is common among well-conditioned runners.
To avoid possible complications such as avascular necrosis, refracture, pseudarthrosis, and prolonged recovery time, early diagnosis of stress fractures is essential.4 Kang, et al, further emphasized that the type of fracture is the most important factor influencing complication rate, with displaced fractures causing the highest rates. Consequently, proper imaging shortly after injury is crucial for detecting early signs of stress fracture.
As the development of stress fracture is considered a continuous process, they may vary in appearance.5 In this regard, the importance of MRI evaluation is highlighted in the literature.6 However, Seki, et al,7 reported the case of a teenaged long-distance runner who suffered a stress fracture of the femoral neck that did not show typical signal changes on MRI. Nevertheless, compared with alternative imaging modalities (CT, radiography, bone scintigraphy), MRI seems the most sensitive and specific imaging approach.8
Adding to the notion that recovery times differ among types of stress injuries, Nattiv, et al,9 proposed a four-grade MRI grading scheme. These grades correlate with risk factors and time to return to sports. Involvement of trabecular structures and subsequent severe bone marrow edema on MRI evaluations (MRI grades 3 and 4), in particular, were associated with significantly prolonged time-to-return to activity.
Further, menstrual dysfunction, low energy availability, and decreased bone mineral density might affect MRI grading severity and are believed to contribute to bone stress injury.9 After other diagnoses such as malignancy have been excluded, pathologic fracture or muscle strain must be considered.10 Additionally, sports-related pubalgia (eg, resulting from secondary or superior cleft injuries) may mimic the pain characteristics of stress fracture but must be treated differently.
With respect to identifying other differential diagnoses, MRI is advantageous to alternative imaging modalities, as it allows a detailed assessment of surrounding tissues. Moreover, Datir, et al,5 pointed out that imaging may help avoid biopsy in many cases. This is of special importance, as stress-fracture biopsies may contain immature cells and osteoid tissue and hence may be misleading.
Conclusion
Stress-related injury of the femur may lead to persistent changes in radiologic exams; rendering a complete clinical picture and correct diagnosis is essential for treatment. MRI evaluation is considered the most sensitive and specific imaging technique for diagnosing stress fracture.
As in the presented case, adding CT may provide a correct diagnosis. An early diagnosis of stress-related fracture is essential for proper treatment and to exclude other differential diagnoses. The presented case also shows that femoral stress fractures may occur in patients without clear risk factors.
References
- Edwards WB, Gillette JC, Thomas JM & Derrick TR. Internal femoral forces and moments during running: implications for stress fracture development. Clin. Biomech. 2008; 23: 1269-1278.
- Warden SJ, Burr DB, Brukner PD. Stress fractures: pathophysiology, epidemiology, and risk factors. Curr Osteoporos Rep. 2006;4(3):103-109.
- Kang L, Belcher D, Hulstyn MJ: Stress fractures of the femoral shaft in women’s college lacrosse: a report of seven cases and a review of the literature. Br J Sports Med. 2005, 39: 902-906.
- Johansson C, Ekenman I, Tornkvist H, et al. Stress fractures of the femoral neck in athletes. The consequences of a delay in diagnosis. Am J Sports Med. 1990; 18:524-528.
- Datir AP, Saini A, Connell A, Saifuddin A. Stress-related bone injuries with emphasis on MRI. Clin Radiol 2007; 62: 828- 836.
- Wall J, Feller JF. Imaging of stress fractures in runners. Clin Sports Med. 2006;25(4):781-802.
- Seki N, Nobutoshi N, Okuyama K, Kam K, Chiba M, Shimada Y. Negative magnetic resonance imaging in femoral neck stress fracture with joint effusion: a case report. 2016. 45(6):843-846.
- Niva MH, Kiuru MJ, Haataja R, Pihlajamaki HK. Fatigue injuries of the femur. J Bone Joint Surg Br. 2005; 87:1385-1390.
- Nattiv A, Kennedy G, Barrack MT, et al. Correlation of MRI grading of bone stress injuries with clinical risk factors and return to play: a 5-year prospective study in collegiate track and field athletes. Am J Sports Med. 2013; 41(8):1930-1941.
- Patel DS, Roth M, Kapil N. Stress fractures: diagnosis, treatment, and prevention. Am Fam Physician. 2011; 83:39-46.
Affiliation: Rostock University Medical Center, Rostock, Germany