Testicular Adrenal Rest Tumors and an Adrenal Nodule in a Patient with Congenital Adrenal Hyperplasia
By Farnsworth P, Schultz E, Rose T


CASE SUMMARY
A 38-year-old male, with a history of congenital adrenal hyperplasia (CAH), presented for management of a recently diagnosed adrenal mass. The mass showed atypical features on imaging and surgical resection was performed. Pathology revealed an adrenocortical adenoma with no adjacent invasion or angiolymphatic spread. Surgery was uneventful, but he subsequently developed bilateral testicular pain and swelling associated with low-grade fevers.
Testicular ultrasound demonstrated a markedly heterogeneous appearance of both testes with multiple hypervascular mass-like areas bilaterally. Infectious workup and tumor markers were negative. It was suggested that the masses were likely related to congenital adrenal hyperplasia secondary to high adrenocorticotropic hormone (ACTH) levels over years which stimulated intratesticular adrenal tissue to proliferate, causing benign adrenal rest tumors. He was placed on testosterone and prednisone daily in order to supplement deficient hormones, secondary to CAH with a slight decrease in the size of his testes. Serial ultrasounds for several years are stable and he has continued to do well.
IMAGING FINDINGS
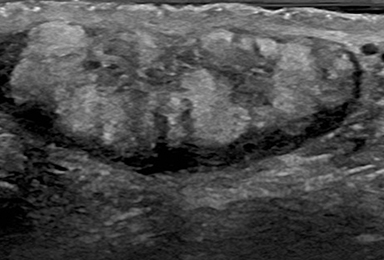
Ultrasound images of the right testis in the sagittal and transverse planes through midline (Figure 1) showed a diffuse, heterogeneous appearance with mass-like areas in the right testis.
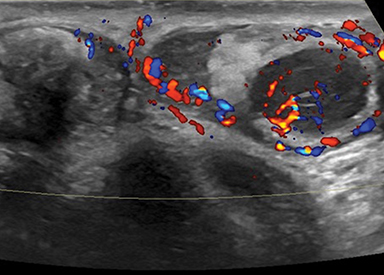
Ultrasound of the left testis in the sagittal plane through midline (Figure 2) demonstrated a heterogeneous appearance with multiple mass-like areas. Also noted is a hypoechoic region within the inferior left testis which has been stable compared to prior exams. A midline sagittal image of the bilateral testes (Figure 2) shows a similar appearance bilaterally with heterogeneous, mass-like areas and internal color flow.
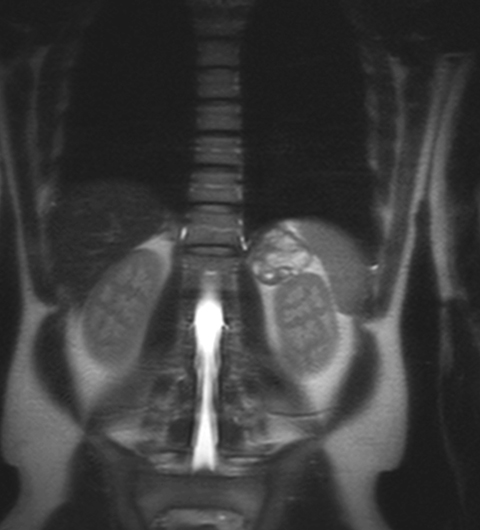
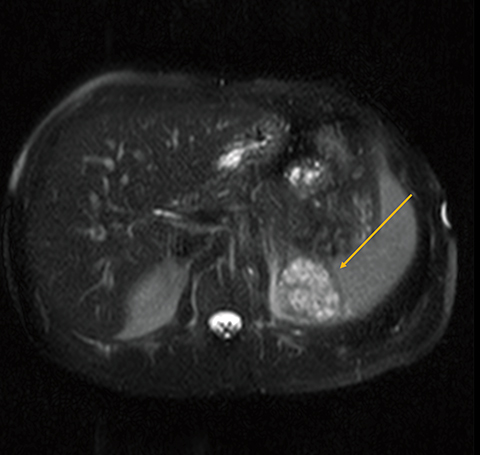
T2 coronal and axial magnetic resonance images (Figure 3) showed a heterogeneous T2 hyperintense left adrenal mass measuring 3 cm (yellow arrow), atypical for adrenal adenoma and suspicious for adrenocortical carcinoma
DIAGNOSIS
Testicular adrenal rest tumors and an adrenal nodule in a patient with congenital adrenal hyperplasia
DISCUSSION
Testicular adrenal rest tumors (TART) are benign tumors that occur secondary to longstanding stimulation of ectopic adrenal tissue within the testis of patients with CAH. CAH represents a group of genetic disorders involving the dysfunction of enzymes in the cortisol biosynthesis pathway.1 The impaired production of adrenal steroids leads to increased secretion of ACTH which, in turn, causes hyperplasia of the adrenal tissue. TART arise from the rete portion of the testis and are remnants of embryonic adrenal tissue that persist into adolescence.2,3
Coexisting adrenal adenomas, as in our patient, are seldom seen in these patients, although a review of the literature reveals that adrenal adenomas also occur due to longstanding inadequate hormone suppression in the setting of CAH.1,4,5,6,7 TART haves been reported in up to 94% of CAH patients; complications include mechanical obstruction, gonadal dysfunction, and infertility.3,5,4,7,8
Owing to the commonly asymptomatic nature of TART, diagnosis is usually not made until the tumors are large enough to be palpated or to cause mechanical obstruction.4,6,7 In patients with known CAH, TART are diagnosed earlier through routine screening, and ultrasound is considered the best, most cost-effective imaging modality for diagnosing TART.
Our case demonstrates the typical ultrasound imaging features of TART; ie, multiple bilateral masses located along the mediastinum testis of varying echotextures with positive color flow on doppler imaging.9 The masses are usually well marginated and can range in size from approximately 0.7 cm to 3.8 cm as reported in one study. They are usually not associated with calcifications. The main differential diagnostic considerations for TART are malignancy (both primary and metastatic disease), infection, and sarcoidosis.
The treatment goals of TART are to reduce the size of the tumors while preserving gonadal function and fertility status. The options for management are glucocorticoid therapy, orchiectomy, or testes-sparing surgery to remove the tumors. Medical management is preferred, as surgery has not been shown to demonstrate a return to normal testicular function or restoration of fertility.2 Prognosis is very good as TART are not malignant.
CONCLUSION
Congenital adrenal hyperplasia is a multifaceted disorder with varying manifestations and levels of severity that can involve multiple organ systems. One complication is testicular adrenal rest tumors. Historically, intratesticular masses have been thought of as most often malignant. However, other etiologies should be considered, especially in patients with a complicated medical history. Here we presented a case of a patient with bilateral testicular masses and an adrenal mass which have a common cause in the setting of congenital adrenal hyperplasia.
REFERENCES
- Tanaka M, Enatsu N, Chiba K, Fujisawa M. Two cases of reversible male infertility due to congenital adrenal hyperplasia combined with testicular adrenal rest tumor. Reprod Med Biol. 2018;17(1):93-97.
- Turcu AF, Auchus RJ. Adrenal steroidogenesis and congenital adrenal hyperplasia. Endocrinol Metab Clin North Am. 2015;44(2):275-296.
- Rohana AG, Ming W, Norlela S, Norazmi MK. Functioning adrenal adenoma in association with congenital adrenal hyperplasia. Med J Malaysia. 2007;62(2):158-159
- Ozisik H, Yurekli BS, Simsir IY, et al. Testicular Adrenal Rest Tumor (TART) in congenital adrenal hyperplasia. Eur J Med Genet. 2017;60(9):489-493.
- Ali HH, Samkari A, Arabi H. Testicular adrenal rest “tumor” or Leydig cell tumor? A report of a challenging case with literature review. Avicenna J Med. 2013;3(1):15-19.
- Chaudhari M, Johnson EK, DaJusta D, Nahata L. Testicular adrenal rest tumor screening and fertility counseling among males with congenital adrenal hyperplasia. J Pediatr Urol. 2018;14(2):155 e151-155 e156.
- Kim MS, Goodarzian F, Keenan MF, et al. Testicular Adrenal Rest Tumors in Boys and Young Adults with Congenital Adrenal Hyperplasia. J Urol. 2017;197(3 Pt 2):931-936.
- Kashyap R. Trails on (18)F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography Leading to Diagnosis of Testicular Adrenal Rest Tumor. Indian J Nucl Med. 2018;33(1):55-56.
- Wang Z, Yang Z, Wang W, et al. Diagnosis of Testicular Adrenal Rest Tumors on Ultrasound: A Retrospective Study of 15 Cases Report. Medicine (Baltimore). 2015;94(36):e1471.
Affiliations: University of South Florida Morsani COM, Tampa, FL (Dr Farnsworth); St. Petersburg General Hospital, St. Petersburg FL (Dr Schultz); Moffitt Cancer Center, Tampa FL (Dr Rose).