Agenesis of the dorsal pancreas



Agenesis of the dorsal pancreas
Findings
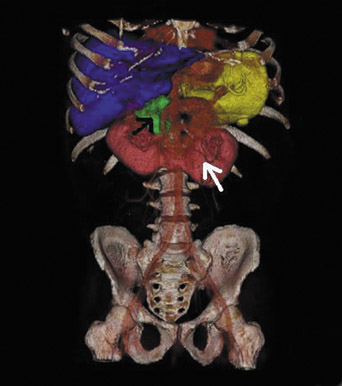
Sonography of the right upper quadrant was unremarkable. A hepatobiliary nuclear medicine scan demonstrated patency of the cystic duct, the study was terminated prior to visualizing activity in the small bowel, and therefore patency of the common bile duct could not be commented on. A computed tomography (CT) study (Aquilion 16, Toshiba America Medical Systems, Tustin, CA) was ordered with 1 mm slices of the abdomen and pelvis acquired using 100 mL of iohexal (Omnipaque™ 300, GE Healthcare, Chalfont St. Giles, U.K.). These images were reformatted in the coronal and sagittal planes as well as reconstructed in 3 dimensions (Figure 1).
Discussion
Agenesis of the dorsal pancreas is a rare anomaly. Patients will commonly present with acute onset abdominal pain and a medical history of diabetes.1 At the time of this writing, 19 cases had previously been described in the literature. To the best of our knowledge, this was the first case occurring in association with the following congenital defects: horseshoe kidney and congenital hydrocephalus. Seven prior cases had previously been described in nondiabetic patients.2,3
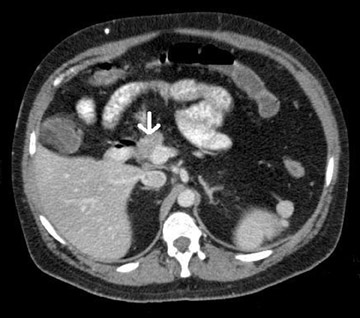
In this patient, CT showed agenesis of the dorsal pancreas (Figures 2, 3 and 4). A uncinate process was present, which had previously been reported as absent in similar cases.4 There was also a congenital horseshoe kidney (Figures 1 and 5). The superior mesenteric artery was seen crossing the transverse portion of the duodenum, though resultant ileus was not seen. Associated findings previously reported, though not seen in this case, are as follows: pancreatic calcifications,4 polysplenia, hepatomesenteric trunk, 2,5 retro aortic left renal vein,5 hypertrophic change of the ventral gland,6 or obvious fatty replacement of the liver. Unlike many other cases of agenesis of the dorsal pancreas, this patient had no history of diabetes mellitus or prior pancreatitis.1,4
The development of the pancreas begins at the fourth week of gestation. Two separate buds arise from the duodenum. The ventral bud originates initially, followed by the dorsal.2 The ventral bud forms the majority of the head and uncinate process. The origin of the uncinate process remains controversial as to whether it arises from the ventral or dorsal pancreatic bud, this case suggests the uncinate process arises from the ventral gland.6 The dorsal bud gives rise to the upper part of the head, isthmus, body and tail. The ventral and dorsal portions fuse at approximately the eighth week of gestation. The dorsal pancreatic duct becomes the major pancreatic duct, emptying into the duodenum via the ampulla of Vater. The proximal portion of the dorsal duct remains patent and becomes the accessory pancreatic duct, draining through the minor papilla. Normally, a communicating channel develops between the 2 ductal systems. When this channel fails to develop, it is termed “pancreatic divisum.”4 If there is agenesis of the dorsal pancreatic bud, a rare anomaly, resultant absence of the body, tail, and uncinate process, as well as the accessory duct of Santorini, and the minor papilla is seen.2 Because the islet cells reside in the tail of the pancreas, the development of diabetes has been attributed to this.1,7 Exocrine pancreatic dysfunction is rare.1
The cause for acute onset abdominal pain is as of yet undetermined. It has been hypothesized that the variant pancreatic duct system may cause insufficient drainage, causing acute, intermittent or chronic pancreatitis.1 However, no findings of pancreatitis were demonstrated in this case.
Conclusion
Advances in multidetector CT, including increased resolution and utilization of isotropic voxels, coupled with the ability to view studies in the sagittal and coronal planes have added another dimension to the diagnosis of congenital anomalies of the pancreas. Whereas in the past, interventional endoscopic retrograde choledochopancreatography was required,3,7 the majority of the cases today can be diagnosed noninvasively.
- Oldenburg B, Van Leeuwen MS, van Berge Henegouwen GP, Koningsberger JC. Pancreatitis and agenesis of the dorsal pancreas. Eur J Gastroentero lHepatol. 1998;10:887889.
- Wang JT, Lin JT, Chuang CN, et al. Complete agenesis of the dorsal pancreas: A case report and review of the literature. Pancreas. 1990;5:493497.
- Fukuoka K, Ajiki T, Yamamoto M, et al. Complete agenesis of the dorsal pancreas. J Hepatobiliary Pancreat Surg. 1999;6:9497.
- Shah KK, DeRidder PH, Schwab RE, et al. CT diagnosis of dorsal pancreas agenesis. J Comput Assist Tomogr. 1987;11:170171.
- Nonent M, Linard J, Leveque E, et al. Dorsal pancreas agenesis: Computed tomography appearance with three dimensional volume rendering reconstruction. Surg Radiol Anat. 2003;25:161163.
- Gold RP. Agenesis and pseudoagenesis of the dorsal pancreas. Abdominal Imaging. 1993;18:141144.
- Wildling R, Schnedl WJ, Reisinger EC, et al. Agenesis of the dorsal pancreas in a woman with diabetes mellitus and in both of her sons. Gastroenterology. 1993;104:11821186.