Pediatric vascular rings and slings
By Evens A, Schaaf W, Anderson J, Neville Kucera J








Vascular anomalies of the aortic arch and great vessels often present in childhood with symptoms related to feeding difficulties or respiratory issues. This review illustrates the appearance of the most common aortic arch anomalies using a multimodality approach including radiography, fluoroscopy, CT, and MRI. The specific entities that will be discussed include double aortic arch, anomalous origin of the left pulmonary artery, right aortic arch with aberrant left subclavian artery, left aortic arch with aberrant right subclavian artery, and innominate artery compression. The different patterns of compression on the esophagus and trachea will be demonstrated. Basic embryology and surgical interventions will also be reviewed.
Double aortic arch
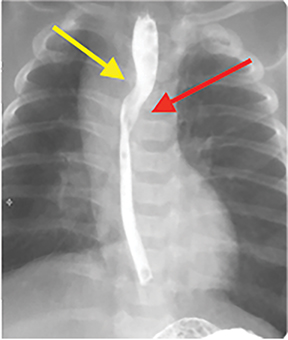
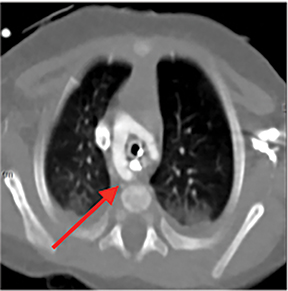
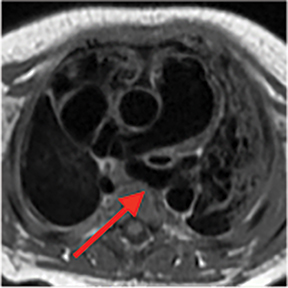
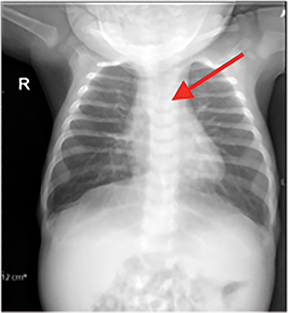
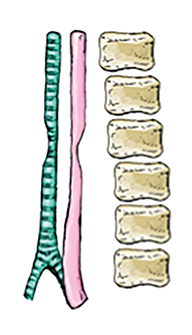
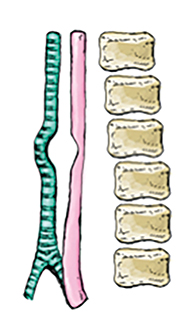
A double aortic arch results from the persistence of the fetal aortic arch system, which includes the right and left fourth aortic arches. The ascending aorta divides into two branches, which encircles the trachea and esophagus, and then reunites on the left to form the descending aorta.1 This anomaly is considered a true vascular ring and produces the most severe symptoms of all the vascular rings. Infants may present with dysphagia or respiratory distress, while there have been case reports of older adults presenting with dysphagia.2 Imaging demonstrates posterior impression on the esophagus and anterior impression on the trachea (Figures 1, 2). Patients who are symptomatic can undergo surgery where transection is directed towards the smaller arch. Of note, more than 80% of patients with this vascular anomaly present with a right-dominant aortic arch.3
Pulmonary sling (anomalous origin of the left pulmonary artery)
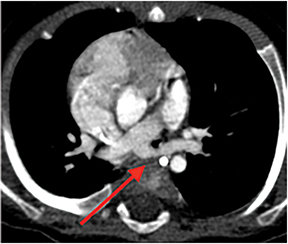
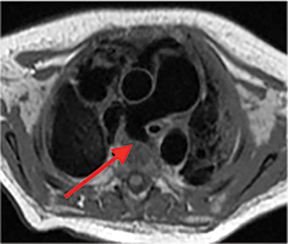
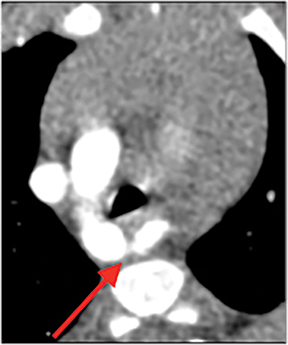
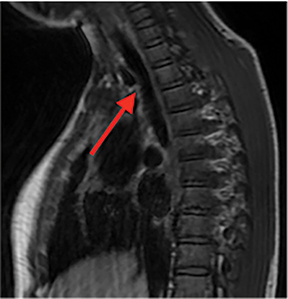
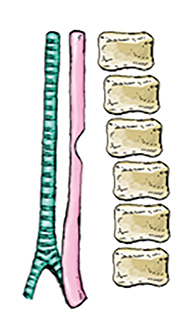
A pulmonary sling occurs from failure of formation of the sixth aortic arch. The left pulmonary artery instead arises from the right pulmonary artery and traverses right to left between the trachea and esophagus. Clinical symptoms are related to narrowing of the right mainstem bronchus and/or trachea, resulting in stridor or atelectasis. Imaging findings typically demonstrate anterior impression on the esophagus and posterior impression on the trachea (Figures 3, 4). There is a high mortality rate without surgical intervention. Repair of a pulmonary artery sling consists of detaching the left pulmonary artery off of the right pulmonary artery and implanting it onto the main pulmonary artery anterior to the trachea.4
Right aortic arch with aberrant left subclavian artery
With this particular anomaly, there is persistence of the right fourth aortic arch with interruption of the dorsal segment of the left aortic arch between the left carotid artery and the left subclavian artery. 3,5 This vascular anomaly infrequently produces symptoms. This is a vascular ring in a majority of cases (90%) secondary to the left ligamentum arteriosum. There are a few types of right aortic arches; right aortic arch with an aberrant left subclavian artery (ALSA) is the most common. This type is associated with a Kommerell’s diverticulum, which refers to the bulbous origin of the left subclavian artery, which represents a remnant of the left dorsal aortic root.3 Chest X-ray typically demonstrates an absent left aortic contour. Sometimes a right paratracheal mass may be seen, which represents the right aortic arch (Figure 5). Other imaging findings include posterior impression on the esophagus (Figures 6). Cross-sectional images demonstrate the aberrant left subclavian artery coursing posterior to the esophagus (Figure 7). Surgery is rarely performed because this infrequently produces symptoms. When performed, surgery involves resecting the Kommerell’s diverticulum and reimplanting the left subclavian onto the left common carotid artery.6
Left aortic arch with aberrant right subclavian artery
The embryology of this vascular anomaly is similar to the right aortic arch with aberrant left subclavian artery, with interruption of the dorsal segment of the right arch between the right carotid and right subclavian artery.5 This is the most common aortic arch anomaly, with an incidence of 0.5-2%, and is not considered a true vascular ring.3 This vascular anomaly is generally asymptomatic; however, a small portion of patients may complain of trouble swallowing, a condition known as “dysphagia lusoria.” Chest x-ray typically is normal. Similar to a right aortic arch with an aberrant right subclavian artery, fluoroscopy demonstrates a posterior impression on the esophagus and cross sectional imaging shows the aberrant right subclavian artery coursing posterior to the esophagus (Figures 8,9). Because symptoms are usually minimal, surgical treatment is rarely warranted.3 If surgery is performed, the aberrant right subclavian artery is divided and anastamosed to the right common carotid artery.7
Innominate artery compression
There is no error in development of the aortic arch. This anomaly can occur if the right innominate/brachiocephalic artery originates more to the left of the trachea than usual. As the artery crosses midline and courses to the right, it can cause anterior compression of the trachea, especially if there is crowding in this region. For example, if the thymus is enlarged or more superior than usual, this may alter the path of the innominate artery.8 It is also important to note that this is not a true vascular ring. If compression of the trachea is severe enough, infants can present with biphasic stridor and respiratory distress. Radiographs are typically normal; however cross sectional images can show anterior compression of the trachea (Figure 10). If symptoms are severe enough, surgical correction is performed with reimplantation/suspension of the innominate artery to the sternum. This procedure is called an “aortopexy.” 9
Figure 11 reviews and illustrates the patterns of compression on the esophagus and trachea from the congenital vascular anomalies described in this article.
Conclusion
Pediatric vascular rings and slings
demonstrate characteristic patterns of compression on images of the esophagus and trachea. Some of these vascular anomalies, such as right aortic arch with an aberrant left subclavian artery and left aortic arch with an aberrant right subclavian artery, are clinically asymptomatic and are incidentally found on imaging. However infants with double aortic arch, pulmonary sling, and innominate artery compression often present with symptoms requiring surgical intervention. Familiarity with these entities is important to ensure accurate diagnosis and management.
References
- Kau T, Sinzig M, Gasser J, et al. Aortic development and anomalies. Semin Intervent Radiol. 2007;24(2):141-152.
- Noguchi K, Hori D, Nomura Y, et al. Double aortic arch in an adult. Interact Cardiovasc Thorac Surg. 2012;14(6):900-902.
- Ramos-Duran L, Nance JW, Schoepf UJ, et al. Developmental aortic arch anomalies in infants and children assessed with CT angiography. AJR Am J Roentgenol. 2012;198(5):W466-474.
- Fiore AC, Brown JW, Weber TR, et al. Surgical treatment of pulmonary artery sling and tracheal stenosis. Ann Thorac Surg. 2005;79(1):38-46.
- Türkvatan A, Büyükbayraktar FG, Olçer T, et al. Congenital anomalies of the aortic arch: evaluation with the use of multidetector computed tomography. Korean J Radiol. 2009;10(2):176-184.
- Chen CL. Repair of right aortic arch with aberrant left subclavian artery and left ligamentum arteriosum. J Pediatr Surg. 1990;25(7):795-796.
- Atay Y, Engin C, Posacioglu H, et al. Surgical approaches to the aberrant right subclavian artery. Tex Heart Inst J. 2006;33(4):477-481.
- Hennington MH, Detterbeck FC, Molina PL, et al. Innominate artery and tracheal compression due to aberrant position of the thymus. Ann. Thorac. Surg. 1995;59(2):526-538.
- Adler SC, Isaacson G, Balsara RK. Innominate artery compression of the trachea: Diagnosis and treatment by anterior suspension a 25-year experience. Ann Otol Rhinol Laryngol. 1995;104(12):924–927.
Dr. Evens is a Radiologist at the University of South Florida Morsani COM, Tampa, FL; and Dr. Schaaf, Dr. Anderson and Dr. Kucera are Radiologists at the University of South Florida Morsani COM, Tampa, FL, and at Johns Hopkins All Children’s Hospital, St. Petersburg, FL. The authors have no conflicts of interest to disclose in relation to this article. This article is based on Evens A, Schaaf W, Anderson J, Kucera JN. Pediatric Vascular Rings & Slings: A Pictorial Review. Oral presentation at: 54th Annual Meeting of the European Society of Pediatric Radiology; June, 2018; Berlin, Germany.