Imaging echogenic breast masses
By Gupta E, Kothari K, McElligott SE





The ACR BI-RADS lexicon describes an echogenic breast mass on ultrasonography (US) as having an echogenicity greater than subcutaneous fat or equal to fibroglandular tissue.1 An echogenic sonographic appearance is attributed histologically to fat, fibrous contents, vascular origin or high cellularity of lesions.2,3
Echogenic breast lesions are uncommon, comprising only 0.6-6% of breast masses and 0.6% of all biopsied lesions.3,4 The majority of these lesions are benign. There are rare malignancies that can present as echogenic masses however, and thorough sonographic assessment according to the ACR BI-RADS criteria must be performed to correctly categorize these lesions and avoid misdiagnosis.
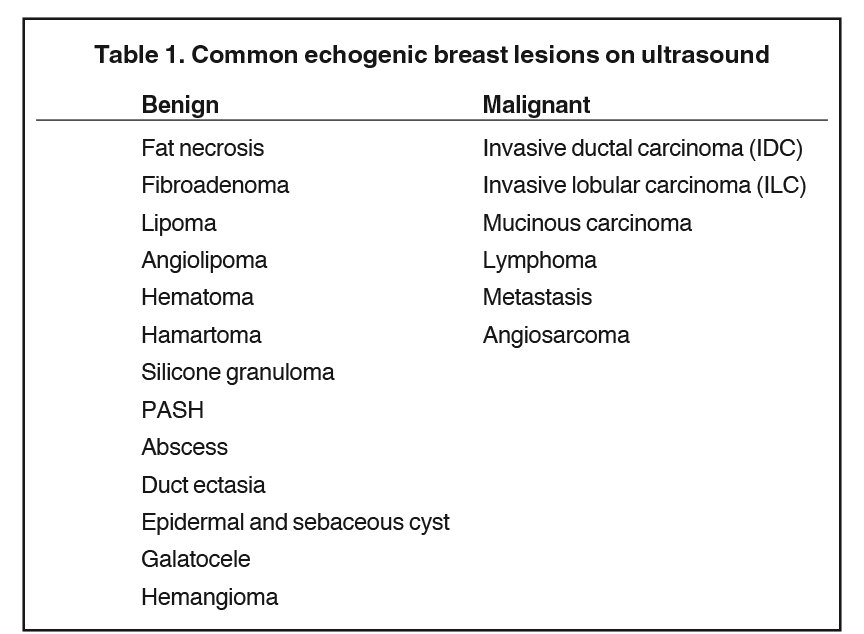
In this article, we will review the imaging features of common benign and malignant echogenic breast lesions on ultrasound (Table 1), emphasizing their correlation with clinical history, mammographic appearance, lesion location and ultrasound features to establish a correct differential diagnosis, determine the need for biopsy and assess the imaging-pathology concordance after biopsy.
Benign hyperechoic lesions
Fat necrosis
Fat necrosis is a common benign entity; it can result from direct trauma, surgery, radiation therapy or infection. On imaging it can mimic malignancy depending on the extent of histiocytic infiltration, hemorrhage, fibrosis, and calcification.2,5
The ultrasound appearance of fat necrosis is variable, ranging from cysts to complex cystic masses to hyperechoic masses.6 On mammography (MG), fat necrosis can present as lipid cysts, calcifications, focal asymmetries, spiculated masses or architectural distortion.4 Careful correlation with the patient’s history and the mammogram findings is prudent to suggest the diagnosis and avoid biopsy (Figure 1).
Fibroadenoma
Fibroadenomas are common benign breast lesions that are composed of stromal and epithelial components, are hormonally sensitive, and more frequent in younger women.3 On US, they typically present as an oval circumscribed mass, and >90% are uniformly hypoechoic. Rarely, they present as hyperechoic (4%) masses (Figure 2).7
Fat necrosis and fibroadenoma were the most frequent observed benign pathologies on ultrasound guided core biopsies of hyperechoic lesions.8
Lipoma
Lipomas are common benign fatty tumors in the breast that are composed of mature lipocytes, usually subcutaneous in location and often unilateral and solitary.2,4 On ultrasound, lipomas can appear as hypoechoic, isoechoic, or hyperechoic masses.4 On mammography, it presents as a radiolucent fat density mass surrounded by a thin fibrous radiopaque capsule confirming benignity (Figure 3).2,4
Angiolipoma
Angiolipomas are composed of mature lipocytes with variable vascular proliferation.9 The pathologic hallmark is scattered microthrombi in small blood vessels.4 On US, angiolipomas are commonly round or oval sub-cutaneous isoechoic to hyperechoic masses with internal vascularity.4,9 Mammography usually shows a dense mass or mixed density asymmetry.4,9 There are no specific imaging features of angiolipomas however, and biopsy is needed for confirmation.4,9
Hematoma
Breast hematoma is a localized collection of blood that can result from direct trauma, surgery, biopsy or rarely occur spontaneously in those with coagulopathy.4,9 The US appearance depends on the age of blood products; it can be hyperechoic from the acute to chronic stages.9 Lipomas, fat necrosis, primary breast cancer and hematologic metastases are in the differential diagnosis of a hyperechoic hematoma.9 Correlation with the patient’s clinical history is essential for the correct diagnosis. A history of trauma favors hematoma. When there is no clear history of trauma or a known extramammary malignancy, a short term follow-up or biopsy may be indicated to exclude malignancy (Figure 4).4,9
Hamartoma (Fibroadenolipoma)
Hamartomas have an incidence of 0.1-0.7% in the breast.3,9 They are composed of variable proportions of fat, glandular and fibrous tissue which determines their imaging appearance.3,9 Frequently they are asymptomatic, but they can present as painless masses. On mammography, hamartomas appear as mixed density (reflecting the fat to stroma ratio), circumscribed masses surrounded by a pseudocapsule.9 At US, these masses are compressible by the transducer and the echo pattern is usually hypoechoic, isoechoic, or mixed echogenicity; but 12-43% of hamartomas appear hyperechoic.3 If it increases in size or density on mammogram or the appearance is atypical, further workup with US and core biopsy are indicated (Figure 5).9
Silicone granuloma (siliconoma)
Siliconoma is an inflammatory mass arising from the presence of free silicone, related to extracapsular rupture or free silicone injection.4,10 On mammography, a silicone granuloma appears as a hyperdense mass of similar density to the silicone implant.4 Ultrasound shows a hyperechoic mass with well-defined anterior margin and posterior dirty shadowing “snowstorm sign” (Figure 6) or an anechoic cystic mass.4,10 Appropriate clinical or surgical history in the setting of aforementioned imaging findings is diagnostic for siliconoma.4
Pseudoangiomatous stromal hyperplasia (PASH)
PASH is a benign proliferative mesenchymal lesion of the breast stroma, seen in perimenopausal women or those receiving hormones.2,3 PASH may present as a rare nodular, and sometimes palpable, form or a diffuse form.2,3 At mammography, PASH can appear as a circumscribed, non-calcified mass or asymmetry. 2,3 At US, PASH often appears as an ovoid or ill-defined, heterogeneous mass and rarely can be hyperechoic.2,3 The imaging features of PASH are not specific, and biopsy is necessary to exclude malignancy (Figure 7).4
Abscess
Abscess is a collection of pus within the breast, usually from mastitis, and presents with pain, erythema and fever.4,11 Abscesses can be classified as “puerperal” (related to childbirth or lactation) or “nonpuerperal”.11 Puerperal abscess are caused by penetration of staphylococcus aureus through a cracked nipple.4,11 Nonpuerperal abscesses are often associated with diabetes, smoking, obesity, and black race and can be subareolar or peripheral.4,11 At US, an abscess may be echogenic, but more often is a complex cystic mass with peripheral vascularity (Figure 8).4,11 Failure to respond to antibiotics and persistence on imaging , should prompt biopsy to exclude inflammatory breast cancer.4,11
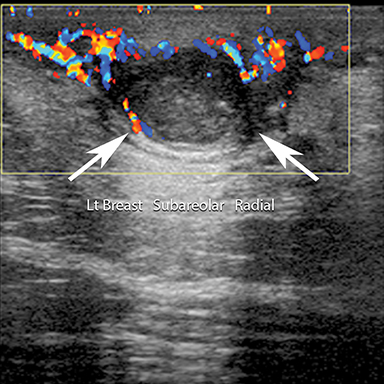
Duct ectasia
Duct ectasia is dilation of the retroareolar ducts from chronic inflammation.4,12 Clinically, it can be asymptomatic or present with nipple discharge. US shows anechoic dilated ducts with or without an avascular intraductal mass.4,12 Intraductal masses can have both benign and malignant pathologies: duct ectasia, fibrocystic change,papillary lesion, DCIS, and IDC.4 Central duct location, multiple similar appearing ducts without internal vascularity, smooth wall and lack of adjacent mass supports a benign pathology.4,12
Epidermal and sebaceous cysts
Epidermal and sebaceous cysts are common dermal lesions and clinically indistinguishable.4,13 Both are retention cysts arising from hair follicles plugged with keratin.13 They are usually palpable and may become inflamed with discharge seen from a small skin orifice.13 US appearance can be cystic, hypoechoic, or echogenic depending on the internal contents (Figure 9).13 Ultrasound demonstration of internal vascularity should prompt biopsy. In contrast, a dermal tract confirms a benign skin lesion.4,13 Needle biopsy of a suspected skin cyst should be avoided as rupture of the cyst can incite an intense inflammatory reaction.13
Galactocele
Galactoceles are milk filled retention cysts caused by blockage of the breast lactiferous duct.4 They are common in pregnant or breast-feeding woman, typically presenting as a painless lump. The mammographic and ultrasound appearance depends on the percentage of fat and protein.14 A galactocele that is predominately milk content has fat density on mammogram and is hyperechoic on US (Figure 10).4,14 Aspiration of a galactocele is both diagnostic and therapeutic, yielding milky fluid.14
Hemangioma
Hemangiomas are common vascular tumors seen in the breast.3,9,15 Pathologically, there are two types: capillary and cavernous (more common subtype) related to the size of their vascular channels on histology.9,15 On US, they are usually superficial, oval, circumscribed masses. Their echotexture may be hypoechoic, isoechoic, or less commonly hyperechoic (33% of cases).3,9,15 The imaging appearance is not specific and biopsy is performed for diagnosis. Excessive bleeding can occur during biopsy, a clue to the diagnosis. Rarely, excision after biopsy is recommended to exclude angiosarcoma.15
Malignant hyperechoic lesions
Although typically hypoechoic, a small subgroup of breast malignancies (0.5%) can present as hyperechoic lesions.4,9,16
Invasive ductal carcinoma (IDC)
IDC is the most common (75%) breast cancer, presenting as an asymptomatic screen detected or palpable mass +/-nipple discharge.3,4 At US, it is classically a hypoechoic mass with non-circumscribed margins; however, in 2% of cases it may be hyperechoic.3,4,17 Echogenic breast masses on sonography with mammographic features such as interval development, spiculated margin, suspicious microcalcifications, or architectural distortion warrant biopsy.4
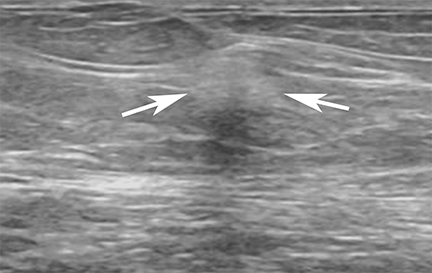
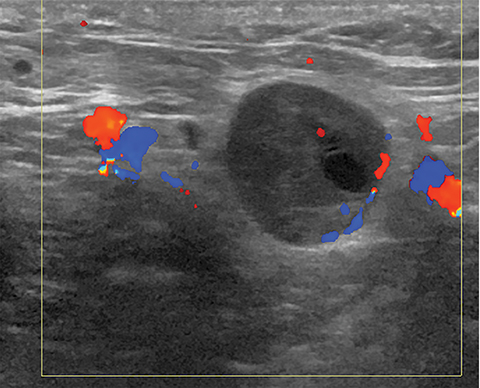
Some invasive breast cancers have a small hypoechoic central focus enclosed by a larger hyperechoic halo. Scanning only through the hyperechoic halo, and not recognizing the central nidus can cause such lesions to be mistaken for a purely echogenic, likely benign finding (Figure 11).18 Additionally, during core biopsy of an echogenic mass with posterior shadowing, care should be taken to biopsy the solid anterior echogenic component.
Invasive lobular carcinoma (ILC)
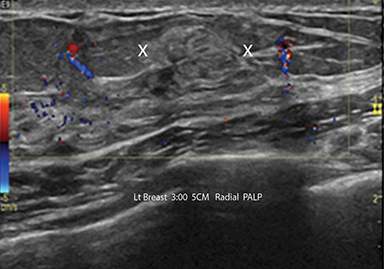
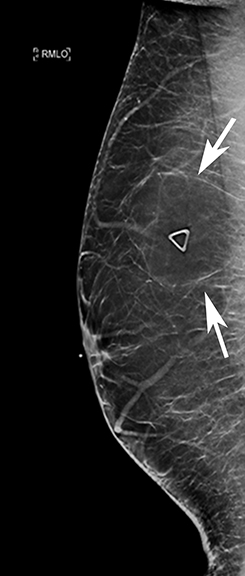
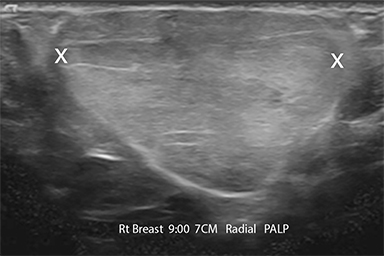
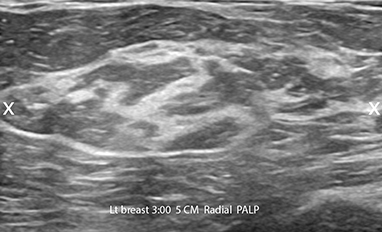
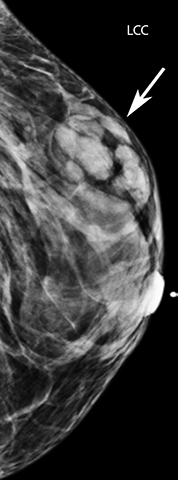
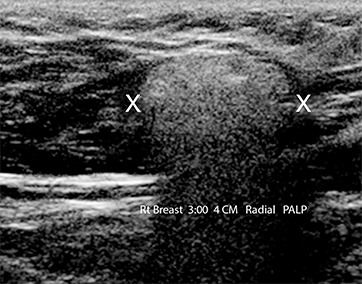
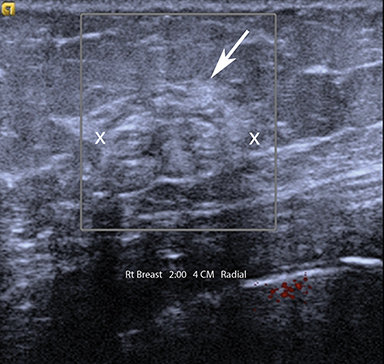
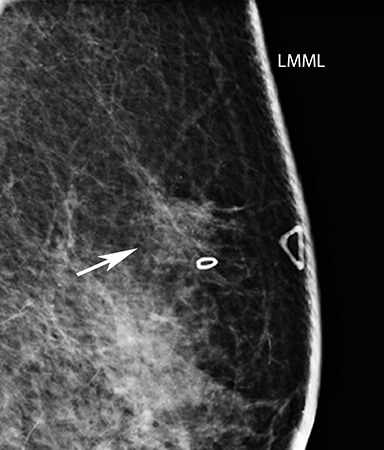
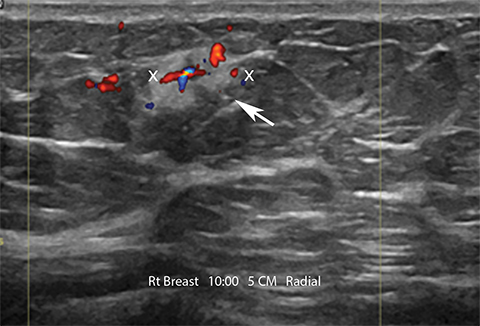
ILC is the second most common (10%) breast cancer.19 Histologically, it infiltrates along the ducts in single rows without a desmoplastic reaction.9,19 The common mammographic appearance is a spiculated mass or architectural distortion (Figure 12A), however ILC can be occult on MG. Features such as absence of a definable mass and hyperechogenicity are relatively frequent on ultrasound (Figure 12B).9,18,19
Hyperechoic lesions are 10X more frequent in ILC, and metastases to the axillary nodes can also appear hyperechoic.9,16 The infiltrative spread of ILC results in more reflective surfaces for the ultrasound beam, the postulated cause of hyperechogenicity.19
Mucinous (colloid) carcinoma
Mucinous carcinoma is a rare breast malignancy, more common in older women.20,21,22 Histologically, it is subdivided into pure or mixed subtypes, depending on the mucin content. The pure subtype has a favorable prognosis with lower incidence of axillary metastasis.18 On mammography, mucinous carcinoma is usually a round or oval, dense circumscribed mass. Ultrasound typically shows an isoechoic or hypoechoic mass, but rarely can be hyperechoic.20,21,22 Ultrasound homogeneity favors a pure subtype, whereas heterogeneity is predictive of mixed subtype with less favorable histological grade (Figure 13).18
Lymphoma
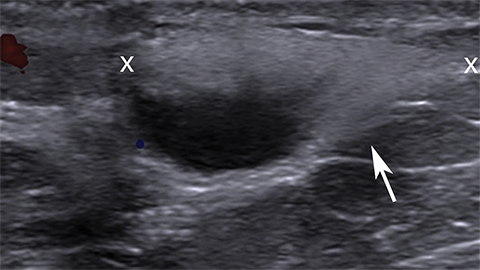
Primary breast lymphoma, where the breast is the only organ affected, is rare.2 The more common secondary lymphoma is associated with extramammary involvement at diagnosis, and the most common subtype is diffuse B cell non-Hodgkin’s lymphoma.9 Lymphoma usually affects older patients, presenting as a palpable mass, sometimes with skin changes, edema and palpable lymph nodes.9,18 Mammogram findings include a circumscribed noncalcified mass, multiple masses or diffuse increased density with skin thickening.9,18,23 On ultrasound, breast lymphomas are typically hypoechoic and frequently hypervascular, less often a mixed echogenic (Figure 14) or echogenic mass.9,18,23
Metastasis
Metastases to the breast are rare, most commonly from melanoma, lung cancer, lymphoma and ovarian cancer.4 A typical presentation is fast growing, painless, palpable masses which can be bilateral.2 Mammography usually shows single or multiple circumscribed masses.2,18 Ultrasound shows hypoechoic or rarely hyperechoic lesions.2,18
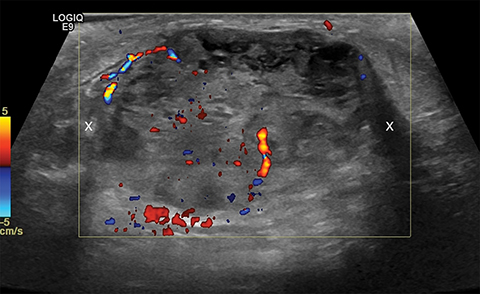
An echogenic mass with internal vascularity requires biopsy, as more than half of breast lymphomas and the majority of melanoma metastases are hypervascular (Figure 15).4
Angiosarcoma
Angiosarcoma is an uncommon breast malignancy of endovascular origin with poor prognosis.24,25 There are two subtypes: primary, occurring sporadically in young women, and secondary, seen following breast cancer treatment in older women with prior history of radiation therapy or post-surgical lymphedema.2,24 Angiosarcomas present as palpable masses or skin discoloration which may be mistaken for bruising, delaying the diagnosis.24 Ultrasound often shows single or multiple, hypervascular, circumscribed or ill-defined hypoechoic masses. However 44% of angiosarcomas can present as mixed echogenic or echogenic lesions (Figure 16).9
Conclusion
Hyperechoic breast lesions, although rare, are not all benign. Occasionally a breast malignancy can present as a hyperechoic mass. The worrisome features in a sonographically echogenic lesion are: irregular shape, non-circumscribed margin, and nonparallel orientation.16 The decision to biopsy should be based on the most suspicious US features, correlation with the mammographic appearance, and the clinical history. When used in conjunction, this knowledge can help the radiologist formulate an accurate differential diagnosis and management plan.
References
- Mendelson EB, Böhm-Vélez M, Berg WA, et al. In: American College of Radiology. ACR BI-RADS® Ultrasound. In: ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System. Reston, VA: ACR; 2013: 59-66.
- Linda A , Zuiani C, Lorenzon M, et al. The wide spectrum of hyperechoic lesions of the breast. Clin Radiol. 2011; 66(6):559-565.
- Medeiros MM, Graziano L, de Souza JA, et al. Hyperechoic breast lesions: Anatomopathological correlation and differential sonographic diagnosis. Radiol Bras. 2016; 49(1):43-48.
- Gao Y, Slanetz PJ, Eisenberg RL. Echogenic breast masses at US: To biopsy or not to biopsy? Radiographics. 2013; 33(2):419-434.
- Taboada JL, Stephens TW, Krishnamurthy S, et al. The many faces of fat necrosis in the breast. AJR Am J Roentgenol. 2009; 192(3):815-825.
- Soo MS, Kornguth PJ, Hertzberg BS. Fat necrosis in the breast: sonographic features. Radiology. 1998; 206(1):261-269.
- Fornage BD, Lorigan JG, Andry E. Fibroadenoma of the breast: sonographic appearance. Radiology. 1989; 172(3):671-675.
- Nam SY, Ko ES, Han BK, et al. Ultrasonographic hyperechoic lesions of the breast: are they always benign? Acta Radiol. 2015; 56(1):18-24.
- Adrada B, Wu Y, Yang W. Hyperechoic lesions of the breast: Radiologic-histopathologic correlation. AJR Am J Roentgenol. 2013; 200(5):W518.
- Brown SL, Silverman BG, Berg WA. Rupture of silicone-gel breast implants: causes, sequelae, and diagnosis. Lancet. 1997; 350(9090):1531-1537.
- Mahoney MC, Ingram AD. Breast emergencies: types, imaging features, and management. AJR Am J Roentgenol. 2014; 202(4):W390-9.
- Ferris-James DM, Iuanow E, Mehta TS, et al. Imaging approaches to diagnosis and management of common ductal abnormalities. Radiographics. 2012; 32(4):1009-1030.
- Geiss C, Raza S, Birdwell R. Distinguishing breast skin lesions from superficial breast parenchymal lesions: Diagnostic criteria, imaging characteristics, and pitfalls. Radiographics. 2011; 31(7):1959-1972.
- Sabate JM, Clotet M, Torrubia S, et al. Radiologic evaluation of breast disorders related to pregnancy and lactation. Radiographics. 2007; 27 Suppl 1:S101-124.
- Jesinger RA, Lattin GE Jr, Ballard EA, et al. Vascular abnormalities of the breast: Arterial and venous disorders, vascular masses, and mimic lesions with radiologic-pathologic correlation. Radiographics. 2011; 31(7):E117-136.
- Nassar L, Issa G, Zarah Z, et al. Predictors of malignancy in hyperechoic breast lesions. J Ultrasound Med. 2016; 35(4):783-790.
- Skaane P, Engedal K. Analysis of sonographic features in the differentiation of fibroadenoma and invasive ductal carcinoma. AJR Am J Roentgenol. 1998; 170(1):109-114.
- Tiang S, Metcalf C, Dissanavake D, et al. Malignant hyperechoic breast lesions at ultrasound: A pictorial essay. J Med Imaging Radiat Oncol. 2016; 60(4):506-513.
- Jones KN, Magut M, Henrichsen TL, et al. Pure lobular carcinoma of the breast presenting as a hyperechoic mass: Incidence and imaging characteristics. AJR Am J Roentgenol. 2013; 201(5):W765-769.
- Memis A, Ozdemir N, Parildar M, et al. Mucinous (colloid) breast cancer: mammographic and US features with histologic correlation. Eur J Radiol. 2000; 35(1):39-43.
- Lam WW, Chu WC, Tse GM, et al. Sonographic appearance of mucinous carcinoma of the breast. AJR Am J Roentgenol. 2004; 182(4):1069–1074.
- Yoo JL, Woo OH, Kim YK, et al. Can MR imaging contribute in characterizing well-circumscribed breast carcinomas? Radiographics. 2010; 30(6):1689-1702.
- Liberman L, Giess CS, Dershaw DD, et al. Non-Hodgkin lymphoma of the breast: imaging characteristics and correlation with histopathologic findings. Radiology. 1994; 192(1):157-160.
- Glazebrook K, Magut MJ, Reynolds C. Angiosarcoma of the breast. AJR Am J Roentgenol. 2008;190(2): 533-538.
- Lim RF, Goei R. Best cases from the AFIP- Angiosarcoma of the breast. Radiographics. 2007;27 Suppl 1:S125-130.
Dr. Gupta is Associate Professor of Radiology at the Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, and Attending Physician; Dr. Kothari is a Diagnostic Radiology Resident at the Donald and Barbara Zucker School of Medicine at Hofstra/Northwell; and Dr. McElligott is Assistant Professor of Radiology at the Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, and Attending Physician. The authors have no conflicts of interest to disclose. This paper was adapted from an electronic educational exhibit, “Echogenic Breast Masses: Why Worry?,” presented by the same authors at the 2017 RSNA Conference in Chicago, IL.