Breast hydatid cysts
By Boski N


CASE SUMMARY
A 60-year-old, postmenopausal female presented with a 1-year history of multiple painless palpable masses of the right breast. The masses had been gradually growing larger, but there was no evidence of associated fever, local tenderness, redness or other skin changes in right breast. There also was no evidence of any palpable enlarged axillary lymph node.
IMAGING FINDINGS
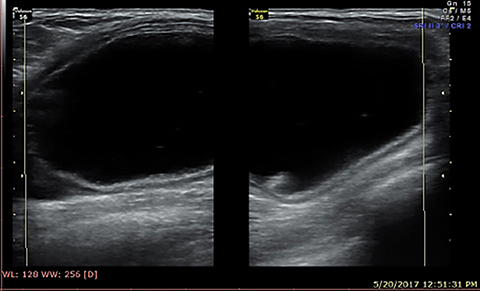
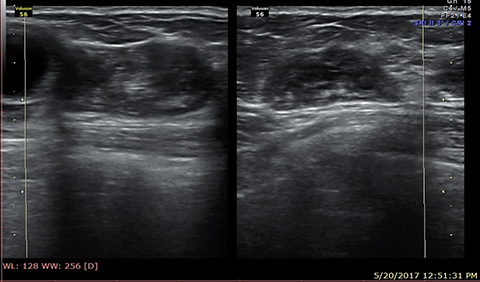
Ultrasound was performed with a high-resolution linear probe. Six lesions with varying internal architecture and sizes ranging from 3 cm to 5 cm in diameter were observed in all quadrants of the right breast. Two cysts were completely internally anechoic with an echogenic wall of 2-4mm thickness (Figure 1). Two other cysts showed thick echogenic walls with multiple, small, daughter cysts. One cyst contained incomplete septations with low-level internal echoes and dependent movable debris (Figure 2). One of the lesions had an echogenic, pseudo-solid appearance with tiny cysts within and a reflecting wall (Figure 3). No obvious ductal dilatation or significant lymphadenopathy was seen. A left breast sonogram, chest radiograph and screening ultrasound abdomen were unremarkable. No further imaging investigations were done. Operative findings were multiple hydatid cysts in varying stages of maturation.
DIAGNOSIS
Breast hydatid cysts
DISCUSSION
Hydatid disease is a parasitic disease caused by multiple species of the Echinococcus genus. Isolated breast hydatid is a rare manifestation1 and multiple hydatid cysts of varying maturation in breast are even rarer. A breast hydatid cyst typically presents as a progressively growing, nontender, palpable breast mass. Clinically, it may mimic various benign and malignant breast masses, such as simple and complicated cysts, abscesses, fibroadenomas, phyllodes tumors, and even carcinoma.2 After physical examination, ultrasound, CT and MR imaging can be performed for diagnosis. Imaging often demonstrates the cystic nature of the lesion, with thick walls and various internal architectures, such as a multicystic (“spoke wheel,” Figure 4) or pseudo-solid appearance, floating membranes (the “water lily” sign), debris (hydatid sand), and peripheral calcifications.
Serological tests like indirect hemagglutination, immune-electrophoresis and ELISA are also used for diagnosis.3
Hydatid cysts have been classified into 5 types by Gharbi:4 a) unilocular cyst with thick wall; b) cyst with detached germinative membrane; c) multicystic appearance with internal septations; d) degenerative pseudo-solid cysts; and e) solid content with calcified wall. This classification has been further refined by a WHO informal working group on echinococcosis to include fertile, transitional, and inactive cysts.5 This classification affects treatment and management recommendations for each cyst type. Depending on the cyst type, treatment options include complete surgical removal or medical and other percutaneous interventional methods. Albendazole has been advised to prevent recurrence. Monitoring is advised for inactive cysts.6
CONCLUSION
Breast hydatid disease is an uncommon but benign entity which, if recognized promptly on imaging, can prevent patient anxiety. Adequate categorization of the cyst into active, transitional, and inactive stages will lead to proper management.
REFERENCES
- Alamer A, Aldhilan A, Makanjuola D and Alkushi A. Preoperative diagnosis of hydatid cyst of the breast: a case report. Pan Afr Med J. 2013; 14:99.
- Karatas T, Kanlioz M and Akin M. Breast hydatid cyst mimicking fibroadenoma and malignancy: A case report. Ulus Cerrahi Derg. 2013;29(3):144-146.
- Krige JEJ and Benckingham IJ. Liver abscesses and hydatid disease. BMJ. 2001; 322:537.
- Gharbi HA, Hassine W, Brauner MW et al. Ultrasound examination of the hydatic liver. Radiology. 1981; 139 (2): 459-463.
- WHO Informal Working Group. International classification of ultrasound images in cystic echinococcosis for application in clinical and field epidemiological settings. Acta Trop. 2003 Feb; 85(2): 253-261.
- Brunetti E, Kern P, Vuitton DA, Writing Panel for the WHO-IWGE. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop. 2010 Apr; 114(1):1-16.
Prepared by Dr. Boski while a consultant radiologist at Sirona Diagnostika, Varanasi, India.