Supernumerary fused kidney
By Arora B, Mishra V, Purohit S
CASE SUMMARY
A 28-year-old woman presented to our hospital with a three-month history of vague upper abdominal pain for which she had been taking NSAIDS. The pain was insidious in onset and non-progressive. On physical examination, the abdomen was soft and non-tender.
IMAGING FINDINGS
A contrast-enhanced CT scan of the upper abdomen was performed. The CECT revealed the left kidney measuring 10.1 × 5.1 cm with non-obstructive calculus measuring 4.5mm in the upper interpolar region, and a calculus of about 2-3 mm in the upper and mid poles. The vascular supply was via a single renal artery and renal vein showing no anatomical variation.
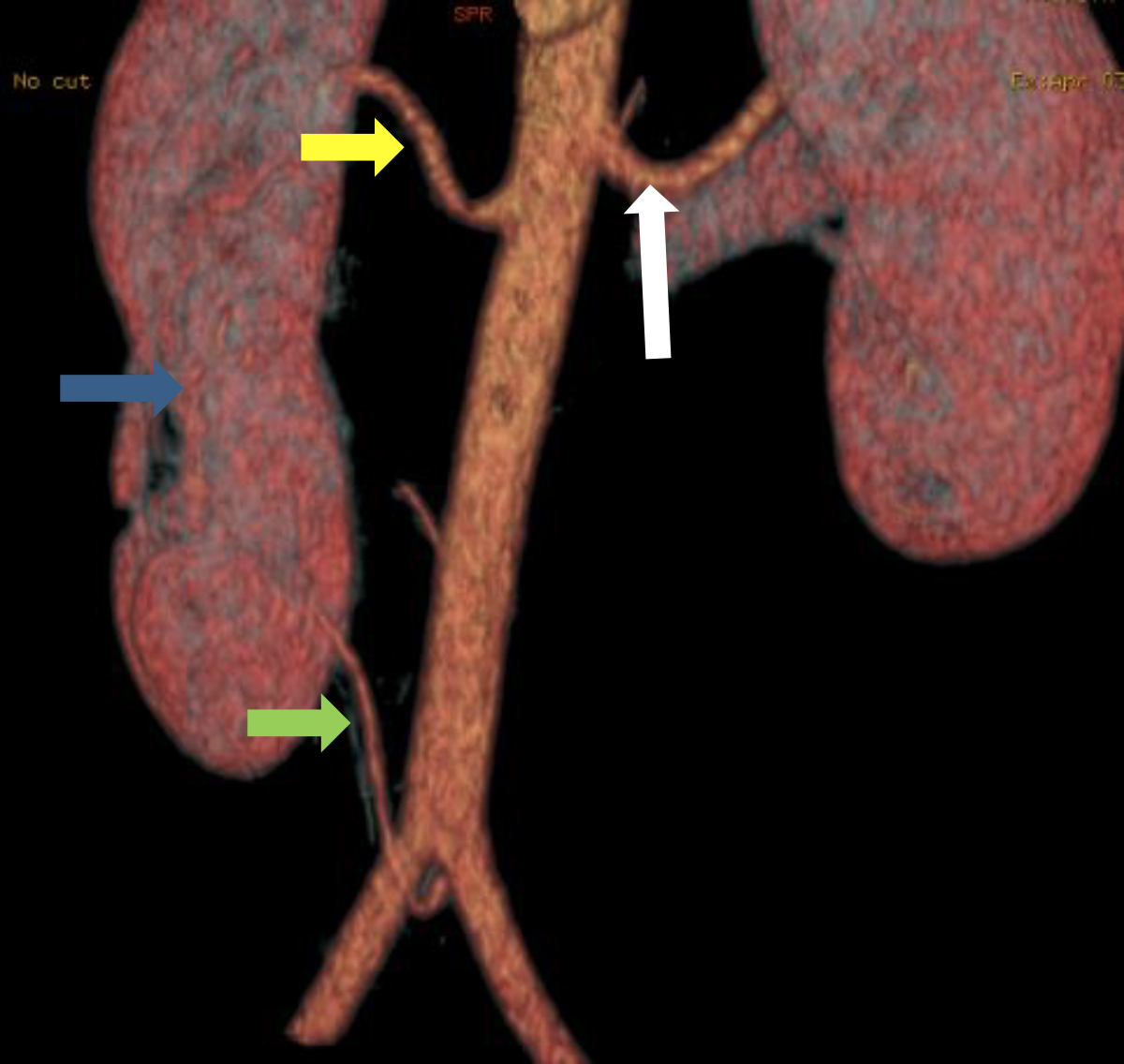
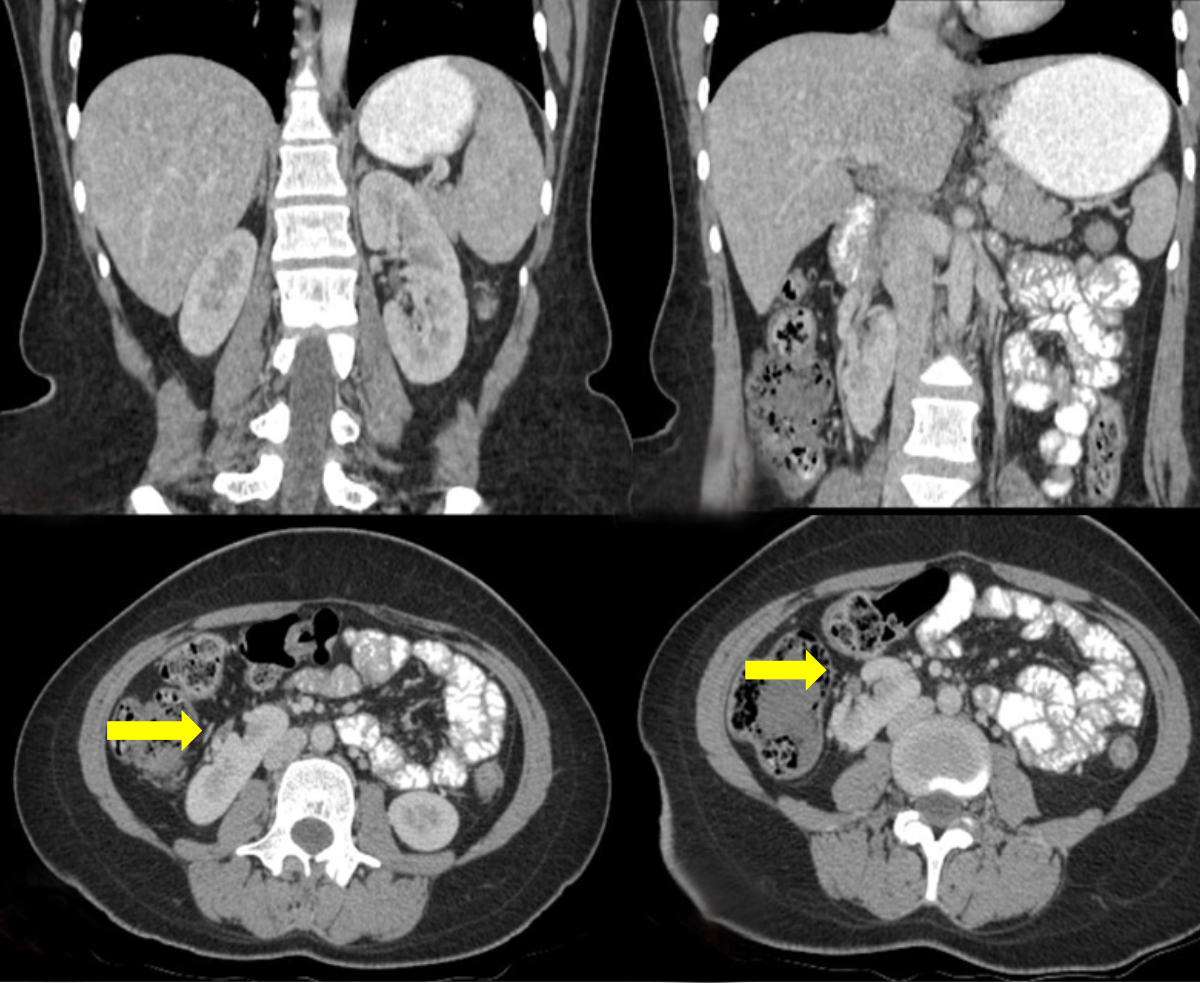
On the right side, meanwhile, the scan revealed two fused kidneys, with the cranially located kidney measuring 8.3 × 3.7 cm, and the caudally located kidney measuring 8.0 × 3.5 cm. These kidneys were partially fused and demonstrated a small parenchymal bridge between them. Two distinct main renal arteries supplied the fused left kidneys. The cranially placed kidney received its arterial supply from a branch of the abdominal aorta. The caudally placed kidney received its arterial supply from a branch of the left common iliac artery (Figure 1). Both the cephalic and caudally placed kidneys drained via renal veins draining separately into the IVC (Figure 2).
The excretory system was normal on left side. However, on right side the renal pelvis of the cranially placed kidney was directed medially, whereas the caudally placed kidney was malrotated with the pelvis directed laterally. Both kidneys on right side were drained by a bifid ureter (Figure 2).
DIAGNOSIS
Supranumerary fused kidneys on right side with tiny renal calculi on left side. Differential diagnosis is duplex kidney.
DISCUSSION:
Supernumerary kidneys are said to be present when the total number of kidneys exceeds two; therefore, supernumerary kidneys can be defined by either the presence of more than two separate kidneys or the observation of an extra kidney coexisting with a horseshoe kidney. A supernumerary kidney can develop from secondary outpouching of the wolffian duct or from branching from the initial ureteral bud; both means of development induce growth of the metanephric anlage, even though the kidneys have separated entirely.1
The supernumerary kidney needs to be differentiated from the more commonly occurring duplex kidney, which is defined as having two pelvicalyceal systems associated with a single ureter or with double ureters. The supernumerary kidney, in contrast, is thought to be an accessory organ with a separate arterial supply, venous drainage, collecting system, and distinct encapsulated tissue. It may be either totally separate from the normal kidney or connected to it by loose areolar tissue acting as a bridge between the two kidneys.2,3 Two types of supernumerary kidney exist: one is drained by a bifid ureter and the other is drained by a separate ureter. When a bifid system is present, the supernumerary kidney lies caudally; however, when a separate ureter is seen, the supernumerary kidney is located cranially in relation to the normal kidney.4
A supernumerary kidney is a rare congenital anomaly of the urinary tract, with fewer than 100 cases documented in the literature, with no difference between the genders and preferential occurrence on the left side. Because of its rarity, the condition typically goes undiagnosed until the fourth decade of life.1,5 Symptoms have been noted in about two-thirds of cases.6 The most commonly associated pathologies include hydronephrosis, pyelonephritis, pyonephrosis, renal and ureteral calculi, carcinoma, papillary cystadenoma, and Wilm’s tumors.7,8
CONCLUSION
Although the patient in this case presented with vague pain, most cases of supernumerary kidneys present with renal symptoms urging prompt medical and surgical attention. As a rare entity, showing variable anatomical features, the condition must be differentiated from the more commonly occurring duplex kidney using imaging findings. Proper description of th enumber, size, position, orientation, vascular supply, and excretory system of the kidneys should be given, in the event surgery is required to address complications like hydronephrosis, pyelonephritis, pyonephrosis, renal and ureteral calculi, etc.
REFERENCES
- Sureka B, Mittal MK, Mittal A, Sinha M, Thukral BB. Supernumerary kidneys: a rare anatomic variant. Surg Radiol Anat. 2014; 36:199–202.
- Tada Y., Kokado Y., Hashinaka Y., et al.: Free supernumerary kidney: a case report and review. J Urol.1981,126: 231-232.
- N’Guessan G., Stephens F.D.: Supernumerary kidney. J Urol. 1983, 130: 649-653.
- Sureka B, Bansal K, Patidar Y. Supernumerary Kidneys Do Exist! American Journal of Roentgenology. 2016 Jan 21; 206(2):W48–W48.
- Suresh J, Gnanasekaran N, Dev B. Fused supernumerary kidney. Radiol Case Reports. 2011;6:552.
- Geisinger JF.Supernumerary kidney. J Urol. 1937; 38:331.
- Antony J. Complete duplication of female urethra with vaginal atresia and supernumerary kidney. J Urol. 1977; 118:877-878.
- Conrad R.G., Loes D.J.: Ectopic supernumerary kidney functional assessment using radionuclide imaging. Clin Nuc Med. 1987, 4: 253-257.