Coronary artery aneurysms
Images
CASE SUMMARY
A 9-year-old girl with known systemic lupus erythematosus (SLE) presents with increasing chest pain. The pain is pleuritic in nature and a pulmonary etiology is suspected.
IMAGING FINDINGS
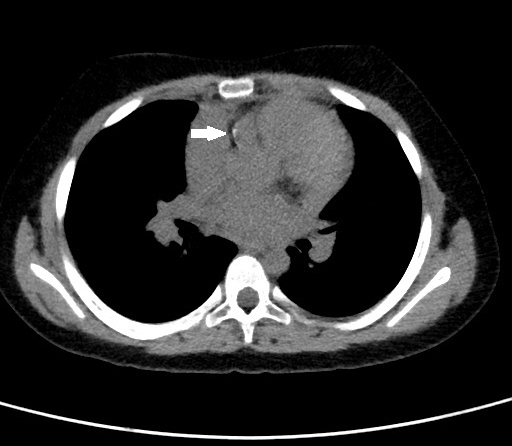
An initial noncontrast CT scan of the chest showed no significant findings within the lungs to explain the patient’s symptoms. However, a soft-tissue abnormality containing a thin rim of calcification was identified within the pre-aortic space (Figure 1). This abnormality was indeterminate, but possible etiologies included vascular or lymphatic abnormalities.
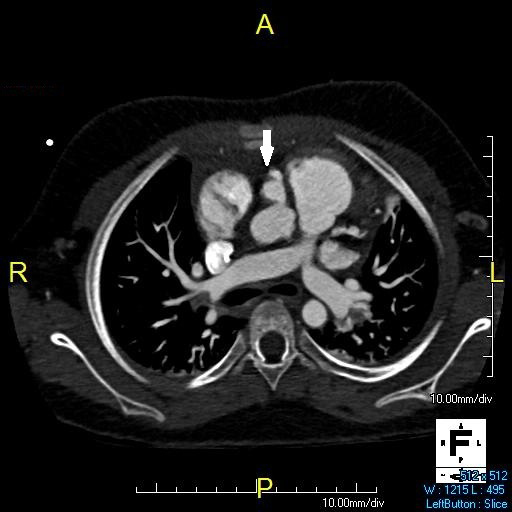
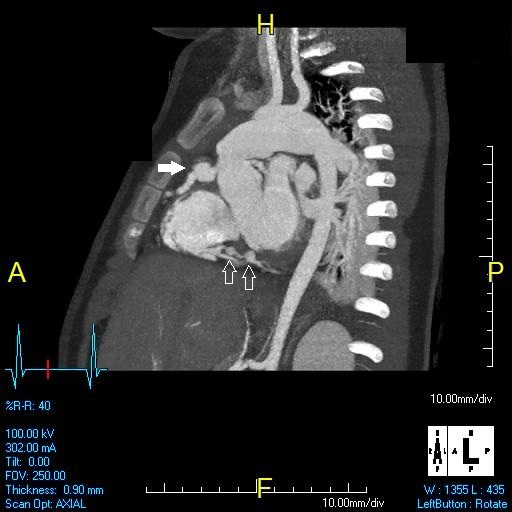
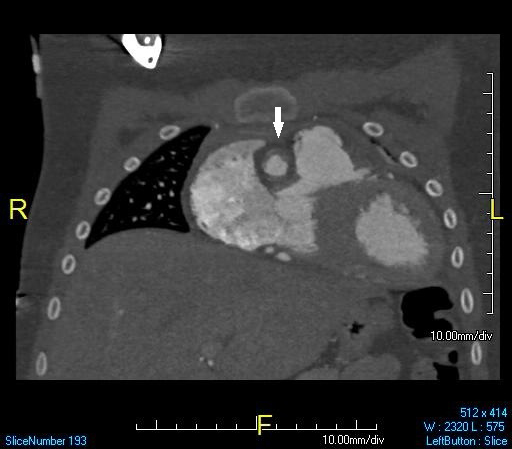
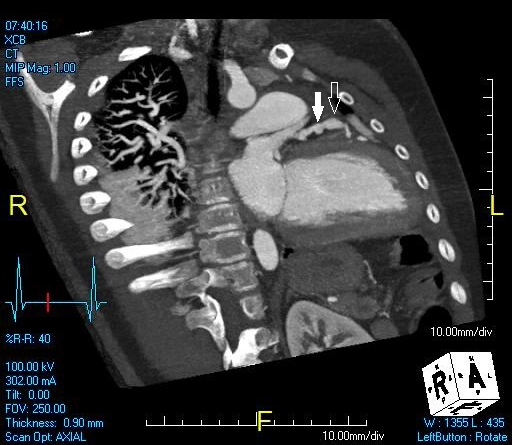
The next day, an ECG-gated, contrast-enhanced CT of the heart was performed. This image showed focal dilatation of the proximal right coronary artery (RCA), just distal to the origin of the artery (Figures 2 and 3) corresponding to the soft-tissue abnormality identified on the non-contrast CT scan. The focal dilatation within the proximal right coronary artery contained a small amount of nonocclusive mural thrombus, as well as a thin rim of calcification (Figure 4). A few smaller areas of focal dilatation were identified within the distal right coronary artery (Figure 3).
Within the proximal left anterior descending artery, there was a small focal dilation as well as a more fusiform dilation located just distally (Figure 5).
DIAGNOSIS
Multiple coronary artery aneurysms secondary to systemic lupus erythematosus
DISCUSSION
Coronary artery aneurysms are a rare complication of a variety of disease processes. Kawasaki disease is the most common cause of coronary artery aneurysms worldwide, particularly in children. Other etiologies include trauma, coronary atherosclerosis, SLE, polyarteritis nodosa, Takayasu’s arteritis, scleroderma, rheumatic fever, bacterial endocarditis, and complications from percutaneous intervention.1
A coronary artery aneurysm is defined as >50% increase in arterial diameter when compared to the adjacent arterial segment;2 they are often asymptomatic. When symptoms are present, they are usually related to myocardial ischemia, such as angina, myocardial infarction, congestive heart failure, or sudden death. Complications from coronary artery aneurysms include thrombosis, embolism, AV fistualization or rupture.2 SLE is a rather uncommon cause of coronary artery aneurysms. Patients with SLE frequently have coronary artery manifestations, with atherosclerosis being much more common than aneurysms. Interestingly, clinical disease activity and serological markers do not seem to correlate well with coronary artery vasculitis or aneurysm.3
The right coronary artery is most commonly affected.1 Catheter angiography historically was used in detecting coronary artery aneurysms, but due to invasiveness and morbidity, as well as technological advances in other modalities, it is performed less commonly now. Echocardiography is commonly used as a screening exam, with excellent visualization of the proximal coronary arteries.4 It can also give valuable data regarding cardiac function to evaluate for complications. With the evolution of multidetector CT, coronary CT angiography (CTA) is becoming more common. Studies have shown CTA to be highly sensitive and specific—and more sensitive than echocardiography for the detection of and demonstration of fusiform and distal aneurysms.2 CTA findings include concentric wall thickening with dilatation of the vessel. Often, a thin rim of calcification can be seen. Coronary stenosis and occlusion are important complications. Hemopericardium can be a clue to aneurysm rupture or impending rupture.
Treatment often varies depending on the etiology of the aneurysm.2 Many patients are placed on aspirin to decrease the changes of thrombosis. Serial exams with echocardiography and/or CT angiography are often performed to evaluate anatomy and function. If stenosis or thrombosis occurs, coronary stenting can be done, though stenosis from vasculitis can be more difficult to stent than stenosis from atherosclerosis. Coronary artery bypass graft surgery is also performed, often with resection of aneurysms.1-4
CONCLUSION
Systemic lupus erythematosus is an uncommon cause of coronary artery aneurysms, with Kawasaki disease being a much more common cause in children. However, children with known SLE who present with chest pain should be evaluated for coronary artery disease, including aneurysms, with echocardiograms or contrast enhanced CT. Treatment varies but can help prevent life threatening complications.
REFERENCES
- Ebina T, Ishikawa Y, Uchida K et al. A case of giant coronary artery aneurysm and literature review. Journal of Cardiology 2009; 53:293-300.
- Johnson P, Fishman E. CT angiography of coronary artery aneurysms: Detection, definition, causes, and treatment. AJR. 2010; 195:928-934.
- Karrar A, Sequeira W, Block J. Coronary artery disease in systemic lupus erythematosus: A review of the literature. Semin Arth Rheum. 2001;30:436-443.
- Newburger J, Burns J. Kawasaki disease. Vasc Med. 1999;4:187-202.
Citation
C W, SA J, AJ T, R T. Coronary artery aneurysms. Appl Radiol. 2015;(6):24-25.
May 31, 2015