Elastofibroma dorsi
Images

CASE SUMMARY
A 75-year-old Caucasian man presented with a palpable right subscapular mass. The patient reported that the mass had been growing for several months, and that pain was elicited upon any movement or motion of his right upper extremity. Upon physical examination, the subcutaneous mass was palpated. It was firm and mobile, and located in the inferior region of the angle of the scapula. The patient reported that pain was elicited upon palpation of the subscapular region, as well as on abduction of his right arm. A chest CT scan without intravenous contrast was then performed, demonstrating bilateral soft tissue masses characteristic of elastofibroma dorsi.
IMAGING FINDINGS
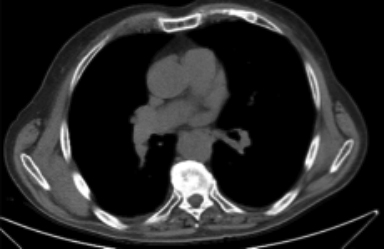
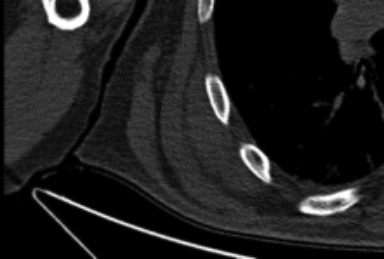
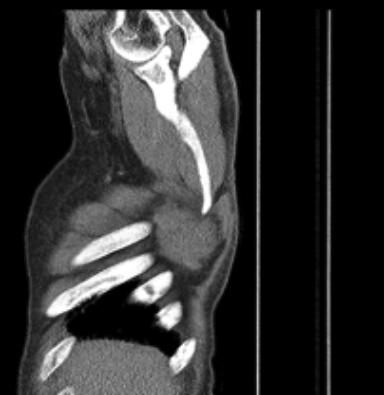
Noncontrast CT demonstrated the presence of soft-tissue masses in the infrascapular region bilaterally, just deep to the anterior serratus and latissimus dorsi muscles, larger on the right measuring 7.1 cm in the AP dimension by 2.5 cm in the transverse dimension, by 6.6 cm in the craniocaudal dimension. These soft-tissue masses were also isodense to the surrounding musculature (Figure 1).
DIAGNOSIS
Elastofibroma dorsi
DISCUSSION
Elastofibroma dorsi is a benign slow growing connective tissue pseudotumor first described by Jarvi and Saxen in 1961.1,2 ED has been shown to be more common in elderly women with an average age of 65, and a prevalence of 2% to 24% in individuals that are older than 55.3,4 Bilateral ED has been observed more frequently, and represents about 30% of cases discovered by CT scan image studies.5
Speculation of the pathogenesis of ED has led to a strong suggestion that recurrent frictional irritation in the region of the angle of the scapula and the thoracic wall yields an increase in propagation of fibroblastic tissue.5 Therefore, occupation may be a risk factor. Studies have shown that ED is more commonly found to be right sided when unilateral, due to right hand dominance. As with patient described earlier, pain is the most common reported symptom. However, ED does tend to be asymptomatic. Affected individuals may also present with a limited range of motion of their upper extremity(ies) as a manifestation of the continued growth of the pseudotumor. Other clinical symptoms include: crepitus, popping or clicking of the scapular region due to contact with the elastofibroma and surrounding anatomical structures.
In a study done by Chandrasekar et al, the composition of the elastofibroma was revealed. Histology provided evidence that elastofibroma is hypocellular, containing a combination of collagen, fibroblasts and elastin with lipoid tissue interspersed centrally.1 This centrally placed adipose tissue allows it to be visualized via CT and MRI imaging. ED commonly presents as a layered appearance when viewed on CT with a soft-tissue or homogenous attenuation.6 Having access to imaging studies has allowed for a more conclusive diagnosis that has helped decline unnecessary testing, biopsies, false diagnosis and successful surgical excision of the elastofibroma.
CONCLUSION
Elastofibroma dorsi is a benign slow growing connective tissue pseudotumor typically found in the elderly population. Its characteristic infrascapular location, soft-tissue or homogeneous central fatty attenuation allows for visualization on imaging. Furthermore, in hopes to enlighten radiologists of this incidental finding, a direct diagnosis can be made on CT when all the above findings are present, with no further need to biopsy the tissue given that the patient is asymptomatic.
REFERENCES
- Chandrasekar CR, Grimer RJ, Carter SR, et al. Elastofibroma dorsi: An uncommon benign pseudotumour. Sarcoma 2008; 1-4. doi:10.1155/2008/756565.
- Ochsner JE, Sewall SA, Brooks GN, and Rashmi A. Elastofibroma dorsi. RSNA. 2006; 26(6): 1873-1876. doi: 10.1148/rg.266055184.
- Naylor MF, Nascimento AG, AD Sherrick, and McLeod RA. Elastofibroma dorsi: Radiologic findings in 12 patients. Am J Roentgenol. 1996; 167(3): 683-87. doi: 10.2214/ajr.167.3.8751681.
- Jarvi OH, Lansimies PH. Subclinical elastofibromas in the scapular region in an autopsy series. Acta Pathol Microbiol Scand A. 1975; 83(1): 87–108. https://www.ncbi.nlm.nih.gov/pubmed/1124654 Accessed August 21, 2016.
- Sarici, Inanc Samil et al. Bilateral Elastofibroma Dorsi: A Case Report. Int J Surg Case Rep. 2014; 5(12): 1139–1141. doi:10.1016/j.ijscr.2014.10.032.
- Brandser EA, Goree JC, and El-Khoury G. Elastofibroma dorsi: Prevalence in an elderly patient population as revealed by CT. Am J Roentgenol. 1998; 171(4): 977-980. doi:10.2214/ajr.171.4.9762978.
Citation
B Y, CC Z, P E. Elastofibroma dorsi. Appl Radiol. 2018;(2):27-28.
February 5, 2018