Glenoid bare spot
Images


CASE SUMMARY
A 14-year-old male competitive swimmer presented with shoulder pain without blunt force trauma after swimming-related activities. The possibility for a labral tear was considered and a magnetic resonance (MR) arthrogram was obtained.
IMAGING FINDINGS
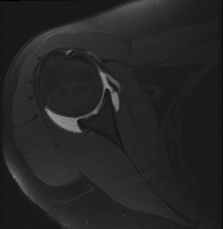
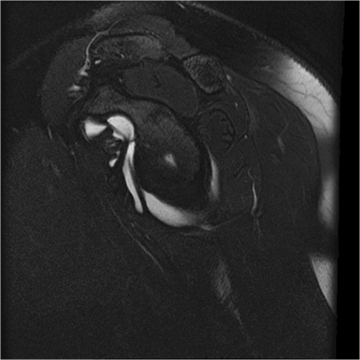
An MR arthrogram was obtained and revealed a 4-mm central area of cartilage loss on the glenoid fossa without underlying bony changes on the axial T1 images with and without fat saturation (Figure 1). This finding was also present on both the coronal oblique T1 (Figure 2) and sagittal T2 fat-saturation images (Figure 3).
DIAGNOSIS
Glenoid bare spot
DISCUSSION
The bare spot of the glenoid fossa is a normal well-marginated cartilage defect that is commonly detected in adults with some reports noting presence in up to 88% of adult cases,1 and is rarely present in children—reportedly found in only 2.1% of children from 11 to 20 years of age, supporting the theory that these may be acquired.1
The glenoid bare spot had been used at arthroscopy as a landmark reference point for the center of the glenoid fossa to determine the presence and size of bony lesions.2 However, this has been noted to be central in only 67% of cases,3 as in our case, thus arthroscopists now consider this as an unreliable landmark for the central portion of the glenoid fossa. Cresswell and colleagues evaluated 50 cadavers, all with no known bone or joint pathology. Both shoulders were dissected and evaluated in these cadavers. In 2 cadavers, there was evidence of bone pathology, and one had a rotator cuff tear on one side. The size of the glenoid and the “bare spot” was measured with a micrometer. The bare spot average diameter was found to be 4.5 mm with a range from 2.4 mm to 9 mm.1 The glenoid bare spot represents the area where the cartilage is thinnest, however, the underlying subchondral bone is not similarly thinned.4
If underlying bone edema is present or if there is any abnormal findings in the underlying bone, then osteochondrosis dessicans or another abnormality should be considered.5
CONCLUSION
The bare spot is seen in children. The absence in children younger than 10-years-old and the low incidence in the second decade support the proposed acquired nature. Familiarity with this finding is important so as not to misinterpret it as a pathologic condition.
REFERENCES
- Cresswell TR, Du Toit D, de Beer JF. The position of the “bare spot” of the glenoid and the relevance to decision making in gleno-humeral instability. J Bone Joint Surg Br. 2005;87-B:167.
- Burkhart SS, DeBeer JF, Tehrany AM, Parten PM. Quantifying glenoid bone loss arthroscopically in shoulder instability. Arthroscopy. 2002;18: 488-491.
- Kim HK, Emery KH, Salisbury SR. Bare spot of the glenoid fossa in children: Incidence and MRI features. Pediatr Radiol. 2010;40(7):1190-1196.
- Schulz CU, Pfahler M, Anetzberger HM, et al. The mineralization patterns at the subchondral bone plate of the glenoid cavity in healthy shoulders. J Shoulder Elbow Surg. 2002;11:174-181.
- Ozturk C, Gogus A. Osteochondritis dissecans of the glenoid cavity: A case report. Arch Orthop Trauma Surg. 2008;128:457-460.
Citation
Glenoid bare spot. Appl Radiol.
September 30, 2013