Neurofibromatosis and atlantoaxial dislocation
Images

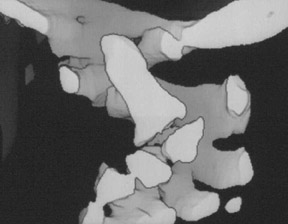

Neurofibromatosis type-1 with atlantoaxial dislocation
Findings
The patient underwent plain X-ray imaging of the cervical spine, computed tomography (CT) of the neck with 3-dimensional reconstructions and magnetic resonance imaging (MRI) of the cervical spine, which showed kyphoscoliotic deformity of the cervical spine with anterior wedging and dysplastic changes of C3 and C4 vertebrae. There was atlantoaxial dislocation (AAD) with predental space of 8 mm and marked reduction of sagittal diameter of the spinal canal at the C1 level (Figures 1 and 2).
Discussion
Neurofibromatosis type-1 (NF1) is the most common of all the phakomatoses, accounting for more than 90% of all cases,1and is the most frequently inherited single-gene disease in human beings.2Two distinct types of neurofibromatosis have been described: NF1 (vonRecklinghausen disease), sometimes termed as peripheral neurofibromatosis, and neurofibromatosis type-2, or central neurofibromatosis. NF1 is an autosomal-dominant congenital disorder in 50% to 60% of cases and arises as spontaneous mutations in the rest. It involves the neural crest cells that affect the development of all 3 germ layers.3,4 It is transmitted on the long arm of chromosome 17 (17q11) and occurs in 1:2500 to 1:4000 live births, has no sex predilection and presents in all groups.5,6 The classic clinical characteristics of NF1 include café-au-lait spots, neurofibroma and several bony anomalies. Involvement of the cervical spine by NF1 is studied infrequently. Our case illustrates many unusual alterations of the cervical spine in patients affected with NF1. The common spinal manifestations of this common phakomatosis are also discussed.
The most common musculoskeletal manifestation in patients of NF1 is scoliosis with an incidence of 71%.7 Involvement of the thoracic spine is the most common, whereas that of the cervical spine has been studied infrequently.3,5 In our case, the thoracic spine was normal with no scoliotic deformity; instead, the cervical spine was predominantly involved.
AAD is rarely reported as part of spinal deformity in patients with NF1, with only 3 case reports available in the literature at the time this document was prepared.7,8 The diagnosis of AAD can be made on plain skiagrams with confidence. Axial CT with 3-dimensional reconstructions provide good delineation of the craniovertebral junction (CVJ). In our case, the predental space was 8 mm on plain skiagrams that was confirmed on subsequent CT and MR images. MRI proved helpful in demonstrating the anatomical changes like the presence of AAD, and other features of mesodermal dysplasia viz, cervical kyphoscoliosis, vertebral wedging, posterior scalloping and duralectasia, that were present in our case.
In neurofibromatosis, osseous tissue that is formed is genetically compromised and is predisposed to erosion and leads to hypoplasia, affecting any part of the vertebral body causing secondary changes such as scoliosis, lateral meningoceles and vertebral scalloping.3 The pathogenesis of AAD in patients of NF1 is not exactly known. However, 2 possible reasons have been speculated: first, being the element of mesodermal dysplasia itself, and second, being the presence of neurofibromatous tissue anterior to the odontoid process.8 In the presentcase, no neurofibroma was found anterior to C2, and since it is a widely accepted fact that in neurofibromatosis there is genetically related maldevelopment of neuroectoderm and mesoderm, there may be associated deformities in the adjacent structures and ligaments—in turn leading to AAD. It is also possible that the ligaments supporting the atlantoaxial joints became misaligned or flaccid, and resulted in AAD.
The characteristic soft-tissue involvement is the development of benign and malignant soft-tissue tumors, most common of which are neurofibromas and schwannomas and include both benign and malignant forms. Approximately 30% of patients with a solitary neurofibroma will have NF1, and virtually all patients with multiple neurofibromas or plexiform histologic findings have the disease.9
Lateral and anterior meningoceles commonly occur in patients with NF1 due to pressure differences between the thorax and subarachnoid space superimposed on bone vertebral defects. Meningoceles usually occur in association with thoracic spine scoliosis.8On CT, they appear as well-circumscribed low-attenuation paravertebral masses because they contain cerebrospinal fluid, and occasionally they exhibit peripheral rim enhancement.
The typical clinical picture of NF1, which is usually identifiable at a glance, consists of multiple hemmed-in areas of increased skin pigmentation (café au lait spots), accompanied by dermal and neural tumors of various types. Occasionally, neurofibromas are found during surgical intervention or incidentally at radiologic imaging.
Conclusion
This case report highlights many issues related to NF1. The most common spinal involvement is witnessed via musculoskeletal presentation. The cervical spine can be rarely involved with normal thoracic spine. Atlantoaxial dislocation is an extremely rare presentation. Plain X-rays are sufficient to diagnose AAD, and other features of mesodermal dysplasia such as, kyphoscoliosis, vertebral wedging and posterior scalloping. CT, and in particular MRI, demonstrate the various associated soft-tissue lesions, e.g. neoplasms, dural ectasia and lateral meningoceles.
- Osborn AG. Disorders of histogenesis: Neurocutaneous syndromes. In: Patterson AS, ed. Diagnostic Neuroradiology. St Louis, Mo: Mosby, 1994;5:72–79.
- Restrepo CS, Riascos RF, Hatta AA, Rojas R. Neurofibromatosis Type-1. Spinal manifestations of a systemic disease. J Comput Assist Tomogr. 2005;29:532-539.
- Tsirikos AL, Ramachandran M, Lee J, et al. Assessment of vertebral scalloping in neurofibromatosis type–1 with plain radiography and MRI. Clin Radiol. 2004;59:1009-1017.
- Shu HH, Mirowit SA, Wippold FJ II. Neurofibromatosis: MR imaging findings involving the head and spine. AJR Am J Roentgenol. 1993;160:159-164.
- Ramachandran M, Tsirikos AI, Leww J, et al. Whole spine magnetic resonance imaging in patients with neurofibromatosis type 1 and spinal deformity.J Spinal Disord Tech.2004;17:483-491.
- Khong P, Goh WH, Wong VC, et al. MR imaging of spinal tumors in children with neurofibromatosis 1. AJR Am J Roentgenol. 2003;180:413-417.
- Veras LM, Castellanos J, Ramirez G, et al. Atlantoaxial instability due to neurofibromatosis: Case report. Acta Orthop Belg. 2000;66:392-396.
- Isu T, Miyasaka K, Abe H, et al. Atlantoaxial dislocation associated with neurofibromatosis. Report of three cases. J Neurosurg. 1983;58:451-453.
- Reed JC, Hallet KK, Feigin DS. Neural tumors of the thorax: Subject review from the AFIP. Radiology. 1978;126:9–17.