Obstructed Hemivagina with Ipsilateral Renal Anomalies
Images

Case Summary
A teenage girl presented with a three-day history of fever and intermittent sharp, stabbing, lower-abdominal pain. The patient’s previous medical history was significant for unilateral polycystic kidney disease with a right nephrectomy and bladder cyst resection in infancy. Additionally, the patient stated that she had menarche at 11 years, with irregular menses. She reported that every other period was heavy and that her last menstrual period ended 4 days earlier.
Imaging
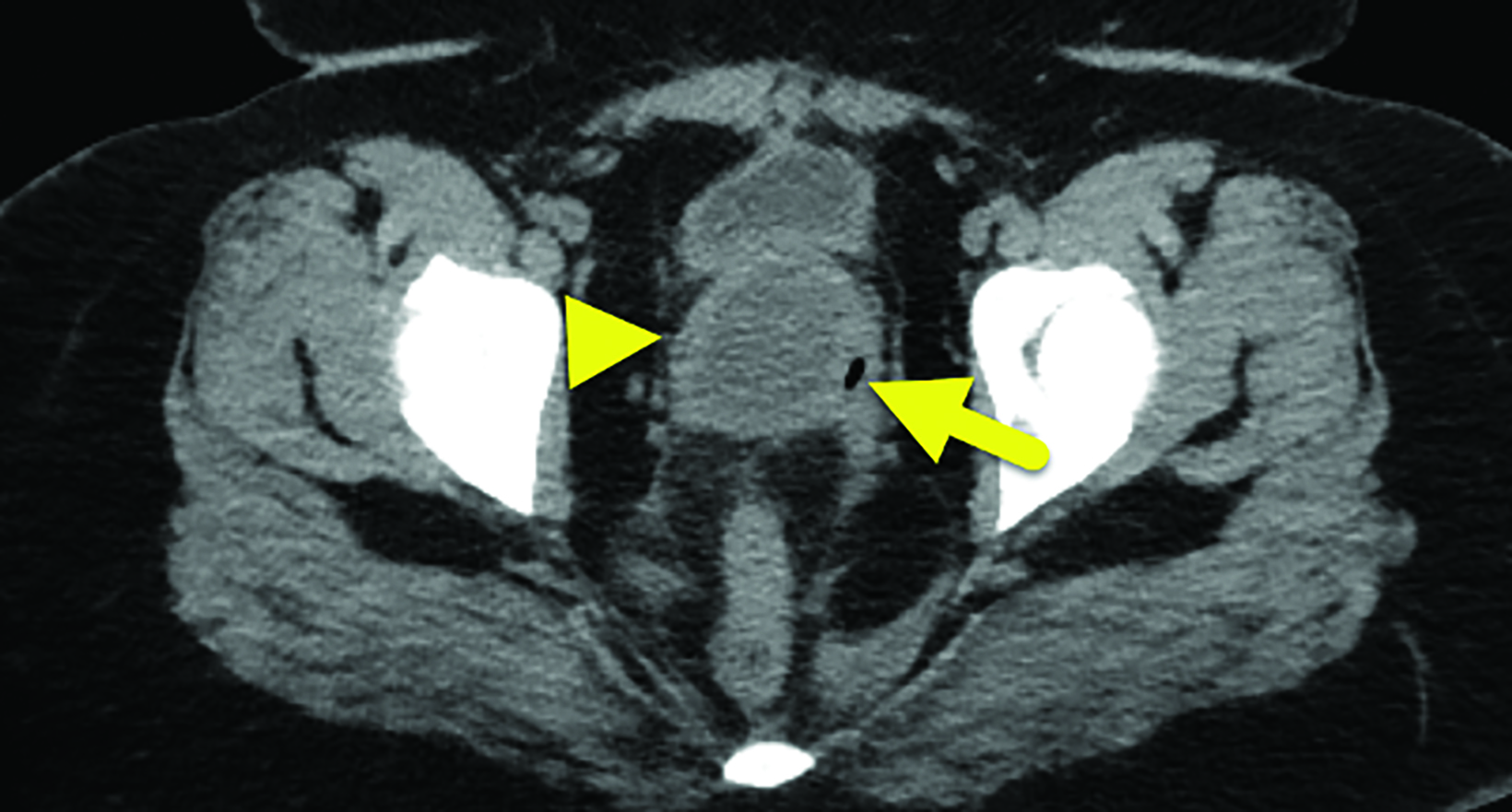
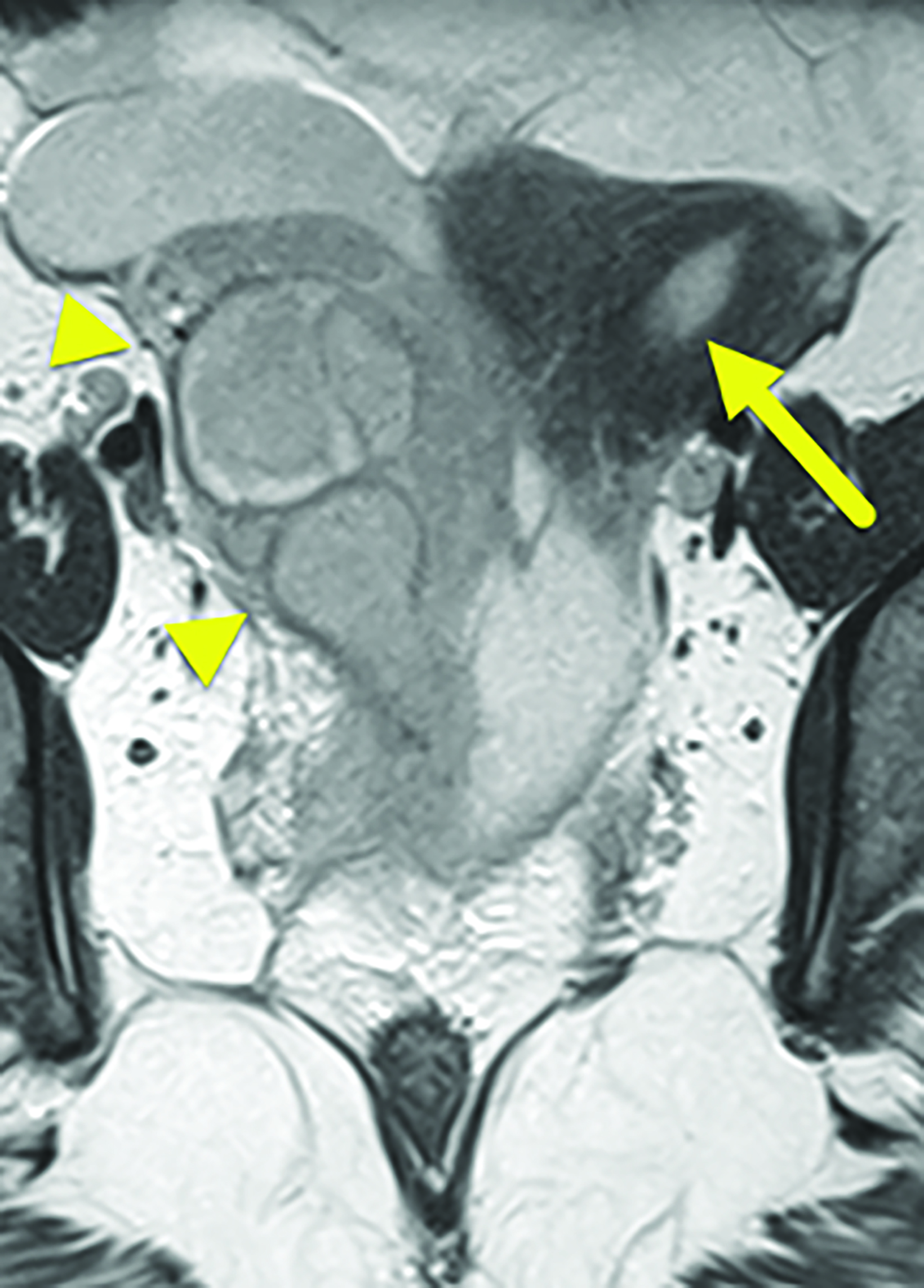
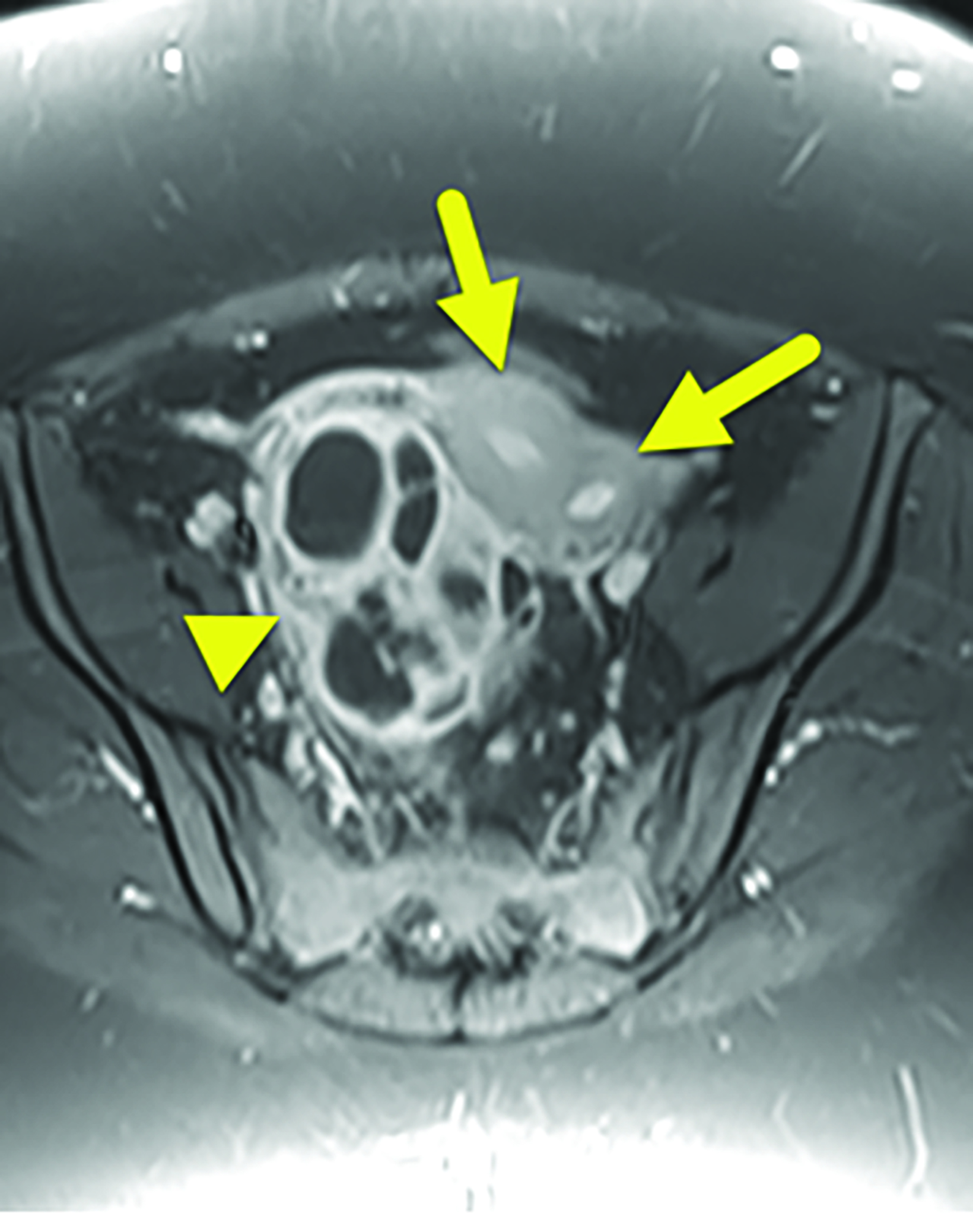
Noncontrast computed tomography (CT) of the abdomen and pelvis (Figure 1) showed a dilated right hemivagina and a fluid collection in the right lower quadrant. Based on the CT findings, the patient underwent pelvic magnetic resonance imaging (MRI, Figure 2). This demonstrated uterus didelphys with a transverse vaginal septum and obstructed right hemivagina. A complex right adnexal tubular and multilobulated cystic abnormality was present with adjacent stranding, suspicious for a right tubo-ovarian abscess.
Diagnosis
Obstructed hemivagina with ipsilateral renal anomalies (OHVIRA), also known as Herlyn-Werner-Wunderlich syndrome (HWW).
Discussion
OHVIRA is a syndrome characterized by the triad of uterus didelphys, an obstructed hemivagina, and ipsilateral renal anomalies.
The condition is also referred to as Herlyn-Werner-Wunderlich syndrome, although this nomenclature is used only when there is unilateral renal agenesis. The incidence is estimated to be 0.1-3% of Mullerian duct abnormalities.1,2
A brief discussion of normal female genital and renal development is necessary to understand the pathology of OHVIRA syndrome.
In normal renal development the mesonephric duct courses from the mesonephros cranially to the urogenital sinus caudally. At about 5 weeks’ gestation, the ureteric bud branches off the caudal mesonephric tubules and contacts a mass of metanephrogenic mesenchyme, beginning the formation of the kidneys.3
Starting at week 4 weeks’ gestation, a gonadal ridge forms within the mesonephros. The gonadal ridge eventually differentiates into the rudimentary ovary. The mesonephros induces the formation of the paramesonephric duct. During week nine, the caudal portions of the right and left paramesonephric ducts fuse to create a uterine septum. The caudal tip of the uterine septum meets mesonephric ducts at the urogenital sinus, forming a clump of paramesonephric cells between them called the Mullerian tubercle.
There are two competing theories regarding subsequent vaginal development: the classical theory and the theory proposed by Acién. According to the classical theory, the vaginal fornices are derived from the paramesonephric duct, and the distal vagina is derived from the urogenital sinus.4
The Acién theory, however, states that while the uterus and cervix originate from paramesonephric ducts, the entirety of the vagina is derived from fused mesonephric ducts and lined by cells of Mullerian tubercle origin. In the latter theory, the cranial mesonephric ducts still regress, but the caudal portions enlarge and eventually form the vaginal cavity.1
OHVIRA can manifest in various ways. Prepubertal diagnosis is now common with the advent of prenatal imaging. Renal abnormalities are often first diagnosed on prenatal ultrasound and most commonly include a multicystic dysplastic kidney and ipsilateral renal agenesis.5,6 The renal anomalies prompt investigation of potential reproductive tract or other urologic anomalies during childhood with ultrasound, MRI, voiding cystourethrogram, and/or MR urography. Potential urologic anomalies include an ipsilateral ectopic ureter, ureterocele, contralateral vesicoureteral reflux, and recurrent urinary tract infections.5
Gynecologic anomalies are typically diagnosed during either infancy or adolescence. Uterine obstruction leading to hematocolpos or hematometrocolpos can be seen in infancy due to stimulation from maternal hormones. This complication may be identified with a renal ultrasound. If not identified during infancy, gynecologic complications may not be diagnosed until adolescence. At that time patients may present with dysmenorrhea and abdominal or pelvic pain caused by the unilateral vaginal obstruction. In some patients, the mass effect caused by hematocolpos or hematometrocolpos may lead to acute urinary retention as a presenting complaint.2
Patients with an obstructed hemivagina may develop an infection leading to complications such as pyocolpos, pelvic inflammatory disease, or tubo-ovarian abscess.7These complications are often first evaluated with ultrasound. The uterine anomalies are then further evaluated with MRI.
OHVIRA is treated with surgical resection of the hemivaginal septum and drainage of hematocolpos.1,5,7If the vaginal septum is thickened, a hemihysterectomy may be performed.7 While patients with Mullerian abnormalities have decreased fertility, successful pregnancies can occur in both the previously obstructed hemiuterus and the nonobstructed hemiuterus.7
Conclusion
OHVIRA is a rare congenital abnormality of the female genitourinary tract characterized by uterus didelphys, an obstructed hemivagina, and ipsilateral renal anomalies. Potential renal anomalies include ipsilateral renal agenesis and multicystic dysplastic kidney. It is most often diagnosed in pubertal females who present with pelvic or abdominal pain resulting from retained blood products. Treatment includes vaginal septum resection with drainage of hematometrocolpos. Although patients have decreased fertility, pregnancy may still be possible in both uteri.
References
- Bajaj SK, Misra R, Thukral BB, Gupta R. OHVIRA: Uterus didelphys, blind hemivagina and ipsilateral renal agenesis: advantage MRI. J Hum Reprod Sci. 2012; 5(1):67-70. doi: 10.4103/0974-1208.97811. PMID: 22870020; PMCID: PMC3409925.
- Jha S, Abdi S. Diverse presentations of OHVIRA syndrome: a case series. Clin Pediatr (Phila). 2021;60(1):6-8. doi: 10.1177/0009922820953582. Epub 2020 Aug 28. PMID: 32856466.
- Acién P. Embryological observations on the female genital tract. Hum Reprod. 1992 Apr;7(4):437-45. doi: 10.1093/oxfordjournals.humrep. a137666. PMID: 1522183.
- Koff AK. Development of the vagina in the human fetus. Contrib Embryol. 1933 24(140):59-91. PMID: 12332362.
- Han JH, Lee YS, Im YJ, Kim SW, Lee MJ, Han SW. Clinical implications of obstructed hemivagina and ipsilateral renal anomaly (OHVIRA) syndrome in the prepubertal age Group. PLoS One. 2016;11(11):e0166776. doi: 10.1371/journal.pone.0166776. PMID: 27861623; PMCID: PMC5115795.
- Smith NA, Laufer MR. Obstructed hemivagina and ipsilateral renal anomaly (OHVIRA) syndrome: management and follow-up. Fertil Steril. 2007;87(4):918-922. doi: 10.1016/j.fertnstert.2006.11.015. Epub 2007 Feb 22. PMID: 17320871.
- Gungor Ugurlucan F, Dural O, Yasa C, Kirpinar G, Akhan SE. Diagnosis, management, and outcome of obstructed hemivagina and ipsilateral renal agenesis (OHVIRA syndrome): Is there a correlation between MRI findings and outcome? Clin Imaging. 2020 Feb;59(2):172-178. doi: 10.1016/j.clinimag.2019.11.013. Epub 2019 Nov 30. PMID: 31821975.
Citation
AR S, RB R, CM S, Y L, AJ T. Obstructed Hemivagina with Ipsilateral Renal Anomalies. Supplement to Applied Radiology. 2022;(6):12-14.
November 2, 2022