Radiation-induced brachial plexopathy
Images



CASE SUMMARY
A 37-year-old male treated with chemoradiation therapy for nasopharyngeal carcinoma (NPC) 11 years prior (radiation dosage to bilateral neck of 5400cGy), presented with progressive upper extremity numbness and weakness. Physical exam revealed decreased upper extremity tone, strength and reflexes bilaterally. Needle electromyography demonstrated myokymic discharges from bilateral del toid, biceps, and triceps.
IMAGING FINDINGS
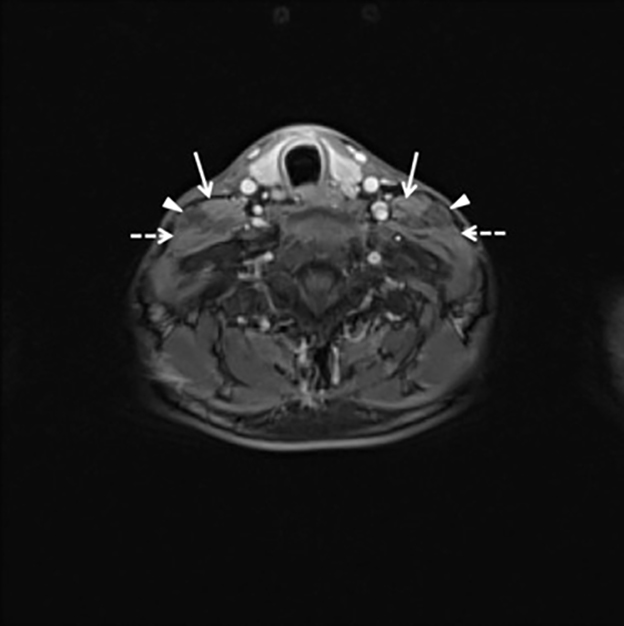
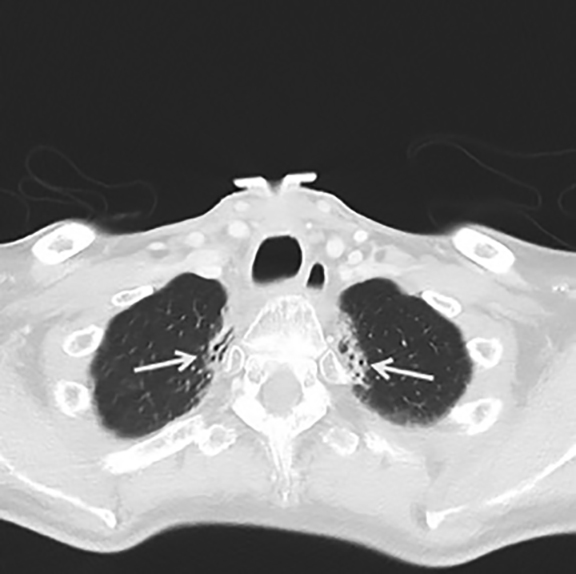
Coronal STIR sequence from a brachial plexus MRI showed marked symmetric thickening and hyperintensity of the brachial plexus roots, trunks, and divisions, in a pattern that matched the radiation treatment port (Figure 1A). The cords and branches (outside the radiation port) appeared normal (Figure 1B). Axial post-contrast T1WI with fat suppression showed thickened right the left brachial plexus with no abnormal contrast enhancement (Figure 2). A contrast-enhanced neck CT performed 7 months prior to the MRI also demonstrated symmetric thickening of right the left brachial plexus (Figure 3) and symmetric bilateral fibrosis of the lung apices (Figure 4).
DIAGNOSIS
Radiation-induced brachial plexopathy
DISCUSSION
Radiation-induced peripheral neuropathy (RIPN) is a rare but relatively well-described complication of radiation therapy (RTX). It was first described in 1966 by Stoll and Andrews.1 The pathophysiology of RIPN is not fully understood, though it is thought that direct nerve injury results from radiation-induced capillary network disruption. This causes ischemia-hypoxia and subsequent axonal damage and demyelination.2 Over time, nerve compression secondary to indirect radiation-induced fibrosis may play a complimentary role.
Radiation-induced brachial plexopathy (RIBP) is one of the best described forms of RIPN and is often seen in patients treated for lymphoma, breast, and lung cancer.2 RIBP incidence is correlated with the irradiation technique and it has become less common over the past 50 years. Studies have shown a mean incidence of RIBP of 1.8-2.9% per year for those who have undergone RTX in the region of the brachial plexus.3,4 Onset of RIBP is often insidious. A case series by Gu et al showed a latency of RIBP after RTX of 1 to 17 years (avg 8.2 years) in 10 patients with nasopharyngeal carcinoma.5 A separate study by Cai et al of 31 patients with RIBP after RTX for NPC showed a mean latency of 4.26 years.6 Our patient first presented with symptoms 11 years after RTX for NPC.
Clinically RIBP begins with subjective parasthesias and pain followed by progressive motor weakness with resulting fasciculations and amyotrophy.6 The specific symptoms vary with the level of plexus damage and the intensity of symptoms is variable. This presentation contrasts with the typical findings of plexopathy secondary to tumor infiltration which often include severe pain, muscle weakness, and occasionally Horner syndrome.7
Magnetic resonance imaging may be required to distinguish between tumor infiltration and RIBP. MR features that suggest RIBP following bilateral RTX include symmetric, bilateral thickening of the nerve roots, hyperintensity of the involved brachial plexus on T2-weighted imaging, and the absence of a focal mass or displacement of adjacent structures.6,8 Mild contrast enhancement may be present making differentiation from tumor infiltration difficult in some cases.9 Electromyography studies can identify the level of plexus injury.10 The nerve conduction in RIBP is normal or slightly reduced compared with frank axonal loss. Myokymic discharges are highly suggestive of RIBP and therefore are of great diagnostic value.2 Our patient demonstrated symmetric thickening of the brachial plexus roots, trunks, and divisions on MRI and myokymic discharges from bilateral deltoid, biceps, and triceps muscles on electromyography.
RIBP ultimately progresses from onset of hand paralysis to full limb paralysis in a range of 0.2 to 5 years.11 The best approach to minimize the risk of RIBP is to limit RTX dose, dose per fraction, and volume.12 Treatment is symptomatic and no cure has been established. Pain related to RIBP can be treated with non-opiod analgesics, benzodiazapines, anti-epileptics, and tricyclic antidepressants. Physical therapy may help maintain function and prevent joint complications. No surgical interventions have proven useful.2 As cancer patients survive longer, the diagnosis and management of late-treatment-related complications, such as RIPB, will increasingly become a health care priority.
CONCLUSION
RIBP is one of the best described forms of RIPN. It is a progressive condition and may develop months to decades after RTX. In severe cases, full limb paralysis may result. There is no cure and treatment is symptomatic. Our patient presented with classic delayed-onset RIBP lower motor neuron deficits with characteristic imaging and EMG findings.
REFERENCES
- Stoll BA, Andrews JT. Radiation-induced peripheral neuropathy. Br Med J. 1966;1:834–837.
- Delanian S, Lefaix J, Pradat P. Radiation-induced neuropathy in cancer survivors. Radiother Oncology. 2012;105:273-282.
- Powell S, Cooke J, Parsons C. Radiation-induced brachial plexus injury: follow-up of two different fractionation schedules. Radiother Oncol. 1990;18:213-220.
- Bajrovic A, Rades D, Fehlauer F, et al. Is there a life-long risk of brachial plexopathy after radiotherapy of supraclavicular lymph nodes in breast cancer patients? Radiother Oncol. 2004;71:297-301.
- Gu B, Yang Z, Huang S, et al. Radiation-induced brachial plexopathy after radiotherapy for nnasopharyngeal carcinoma. Jpn J Clin Oncol. 2014;44:736-742.
- Cai Z, Li Y, Hu Z, et al. Radiation-induced brachial plexopathy in patients with nasopharyngeal carcinoma: a retrospective study. Oncotarget. 2016;7(14):18887-18895.
- Kori SH, Foley KM, Posner JB. Brachial plexus lesions in patients with cancer: 100 cases. Neurology. 1981;31:45-50.
- Bowen BC, Verma A, Brandon AH, Fielder JA. Radiation-induced brachial plexopathy: MR and clinical findings. AJNR. 1996;17:1932-1936.
- Iyer VR, Sanghvi DA, Merchant N. Malignant brachial plexopathy: A pictorial essay of MRI findings. Indian J Radiol Imaging. 2010;20(4):274-278.
- Mondrup K, Olsen NK, Pfeiffer P, Rose C. Clinical and electrodiagnostic findings in breast cancer patients with radiation-induced brachial plexus neuropathy. Acta Neurol Scand. 1990;81:153-158.
- Fathers E, Trush D. Radiation-induced brachial plexopathy in women treated for carcinoma of the breast. Clin Rehabil. 2002;16:160-165.
- Delanian S, Lefaix J-L. Current management for late normal tissue injury: radiation-induced fibrosis and necrosis. Semin Radiat Oncol. 2007;17:99-107.
Citation
G M, M H, SH P. Radiation-induced brachial plexopathy. Appl Radiol. 2017;(6):20-22.
June 8, 2017