Breast-Specific Gamma Imaging

While mammography remains the gold standard for breast cancer detection, its findings can, at times, be inconclusive, particularly in women with dense breast tissue or changes within the breast parenchyma. "For women with dense breast tissue, cancer screening can be very challenging," said Nathalie Johnson, MD, Medical Director of the Legacy Breast Health Centers and an oncology surgeon at the Legacy Good Samaritan Hospital & Medical Center, Portland, OR. For these patients, magnetic resonance (MR) imaging is often included in the diagnostic workup due to its higher sensitivity. However, published studies indicate that the specificity of breast MR varies, potentially resulting in false-positive findings.
"As a surgeon taking care of breast cancer patients, my frustration has been that the sensitivity of MRI is great but its specificity could be better," said Johnson. "Because of MRI's high false-positive rate we do more biopsies than are necessary, or, in some cases, women elect for mastectomy when they could have had breast-conserving therapy."
Breast-Specific Gamma Imaging (BSGI) with the Dilon 6800 Gamma Camera (Dilon Technologies, Inc., Newport News, VA) provides the same high sensitivity of MR but with a much higher specificity. "With BSGI we have the same sensitivity as MR but a better specificity," said Johnson. "That, to me, is what is exciting about BSGI."
Sensitivity/Specificity of BSGI
"BSGI is both very sensitive and very specific," explained Margaret Bertrand, MD, Medical Director of the Bertrand Breast and Osteoporosis Center (Greensboro, NC), which recently became a part of Solis Women's Health of Austin, TX. "In my experience, BSGI has been 90% specific and, in my first 50 cases of confirmed cancer, its sensitivity has been 92% to 96%."
"We just finished reviewing our first 170 cases," added Johnson. "With BSGI, we had a biopsy rate of about 5%. If you calculate what you would expect with MR, we probably would have had a biopsy rate of about 14%. Of that 5%, 50% were cancers. So far, BSGI has given us fewer positives than MR, and, in cases where its findings have been positive, there was a very high likelihood that there was a malignancy."
This high level of sensitivity can be especially helpful in patients who may wish to take a wait-and-see approach, explained Bertrand. "Some women are in denial," she said. "I show them the mammographic findings, but they say they do not want to have a biopsy or MR imaging. With BSGI, it's nice to be able to tell patients that I have an easy test that they can do and if its results are positive, there is a greater than 90% chance that it is cancer."
The Patient Experience
For the patient, the exam is much easier than MR imaging as well. "There is a big difference for the patient," said Bertrand. "With MR imaging patients have to lie on their stomachs, which some women find very uncomfortable. I've also had numerous claustrophobic patients who have refused to try MR, even with sedation, and 2 who agreed to try it with sedation who couldn't go through with it when the time came. I've also had a patient who had a brain aneurysm repair and had a clip at the site, a contraindication to MRI."
"BSGI, on the other hand, is very comfortable," continued Bertrand. "The patient sits throughout the exam; most of my patients read a magazine while they are having it done." The entire exam takes approximately 45 minutes. Each breast is imaged in the same position as a mammogram is performed, resulting in images that can be easily compared to the mammographic findings.
Case Report - Multifocal Disease
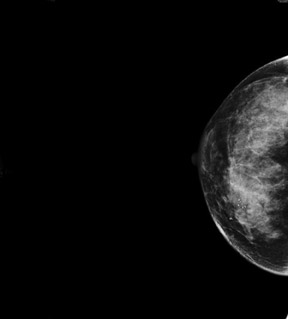
A 48-year-old woman with dense breast tissue and a prior negative biopsy reported dimpling in her right breast near the nipple. Mammographic findings revealed no mass or spiculation and no significant changes from 2 years prior (Figure 1). Ultrasound examination showed a hypoechoic area thought to be scarring from the earlier procedure. The patient was asked to return for follow-up in 6 months, but returned in 8 weeks, reporting an increase in the dimpling.
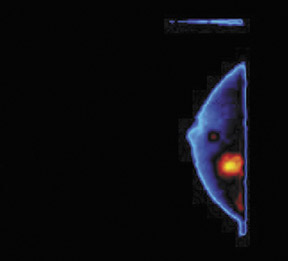
Follow-up ultrasound noted fibrocystic change but no discrete mass. BSGI was performed, and a 2-cm area of increased uptake was noted in the upper-inner quadrant of the breast (Figure 2). A 1-cm area of more intense focus was noted at the 6 o'clock position. There was also increased activity in the right axilla. BSGI findings for the left breast were negative.
Following BSGI, MR imaging was performed. The lesion at the 6 o'clock position on her right breast clearly enhanced and there was mild, non-specific enhancement at the 12 o'clock position in the same breast. The MRI also showed some enhancement in the left breast. A needle biopsy on the lesion at 6 o'clock in the right breast confirmed the presence of infiltrating ductal carcinoma. A generalized core biopsy was performed at the 12 o'clock position, the findings of which were considered to be benign. A repeat MRI was performed on the left breast with the intention of doing an MRI-guided needle biopsy, but no lesion was seen at that time and the initial MR results for her left breast were considered to be a false positive.
A lumpectomy at the 6 o'clock position was performed, and a 1.2-cm moderately differentiated ductal carcinoma was removed. A localized excision of the area of focal uptake on BSGI in the upper-inner quadrant was also performed, and a 2-cm DCIS (Ductal Carcinoma in Situ) and positive axillary nodes were confirmed.
In this case, BSGI detected multifocal disease in a patient with negative findings on both mammogram and ultrasound while MR indicated showed enhancement in an area later confirmed by pathology to be negative.
Case Report - Lobular Carcinoma
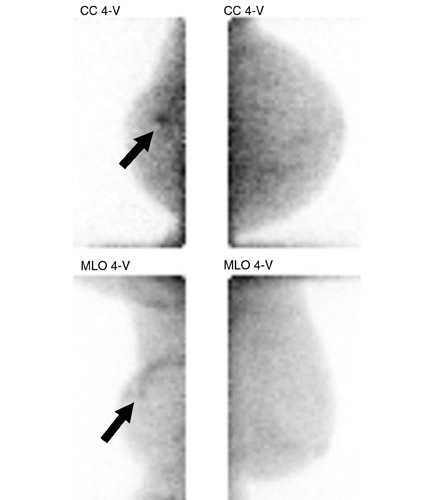
A 59-year-old woman presented with deformity of the left breast due to lumpectomy and radiation therapy for breast cancer 8 years prior. Ultrasound examination at the lumpectomy site showed a pattern of focal hypoechogenicity consistent with scar tissue but the presence of an underlying tumor could not be excluded. BSGI examination revealed a 7-mm area of abnormal isotope uptake (Figure 3). Repeat ultrasound showed only a blackout from the scar tissue.
With MR imaging (Figure 4), the entire scar tissue enhanced; however, a small area of additional enhancement was noted in the area corresponding to the finding on BSGI. MR-guided biopsy was performed based on the BSGI findings and invasive lobular carcinoma was diagnosed. The patient underwent mastectomy, and the only cancer found was the 7-mm area seen with BSGI. In this case the MR results were non-specifically positive, but the BSGI, which was focally positive, allowed the radiologist to target the specific area of concern for biopsy.
Conclusion
"I don't think there is going to be one single breast imaging modality that is 100% accurate all the time in picking up breast cancer, at least not in my lifetime" said Bertrand. "I think it's going be a combination of imaging modalities, and our goal, at least for the next few years, should be to narrow that down to the most accurate and cost-effective methods of diagnosing breast cancer."
"From my practice experience," she concluded. "BSGI is an optimal adjunctive screening tool to mammography for some high-risk patients, and may be better than MRI for screening because it is more accessible, faster, easier on the patient, and more affordable ."