Pediatric urinary tract emergencies
Images







Urinary tract conditions are a frequent cause of acute signs and symptoms in infants and children resulting in presentation to the emergency department. The imaging evaluation of these conditions strongly impacts the diagnosis and patient management. Therefore, selection of an appropriate imaging strategy and knowledge of the typical imaging appearance of common urinary tract emergencies is essential to ensure prompt treatment. This article focuses on the important clinical and imaging features of common urinary tract emergencies in children.
Posterior urethral valves
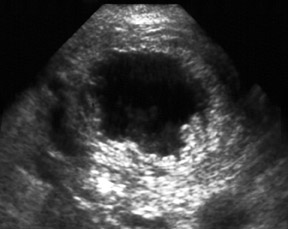
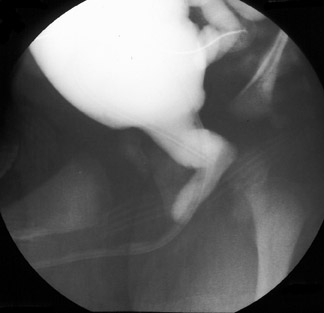
Posterior urethral valves result from redundant folds of urethral tissue in the posterior urethra, which lead to obstruction of urinary outflow. The folds attach immediately below, above, or at the verumontanum. Posterior urethral valves are the most common cause of lower urinary tract obstruction and the leading cause of end-stage renal disease in boys. The diagnosis is often made at prenatal imaging, but it is not unusual for the condition to be initially diagnosed after birth. Clinical findings include a palpable abdominal mass representing enlarged kidneys and/or bladder, voiding abnormalities, or symptoms related to urinary tract infection. The initial imaging examination performed is typically sonography, which shows bilateral hydroureteronephrosis and a dilated and/or thick-walled bladder (Figure 1).1 The dilated posterior urethra may also be seen by using the distended bladder as an acoustic window or with transperineal scanning.2 Variable degrees of renal parenchymal thinning are typically seen. Additionally, renal dysplasia is a common complication from prolonged obstruction that resuls in increased renal parenchymal echogenicity and parenchymal cysts. These findings typically indicate irreversible renal insufficiency. The diagnosis of posterior urethral valves is confirmed with voiding cystourethrography (VCUG). The findings at VCUG include a dilated posterior urethra with diminution of the urethral caliber distal to the valves (Figure 2). The bladder capacity is often small, and the bladder wall may be trabeculated. Vesicourethral reflux is also commonly seen at VCUG in association with posterior urethral valves.
Ureteropelvic junction obstruction
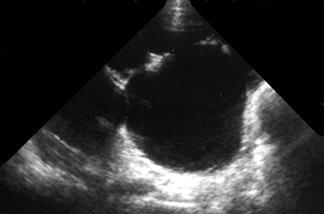
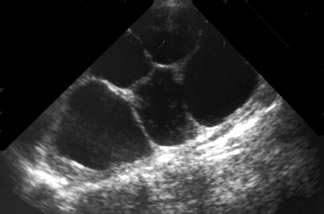
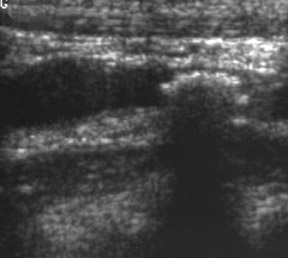
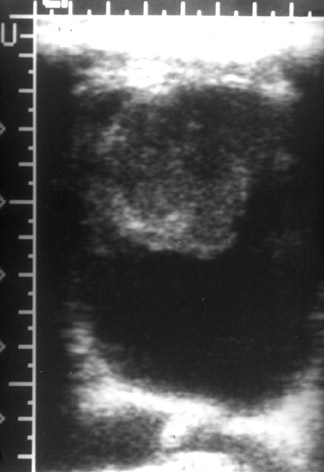
Ureteropelvic junction (UPJ) obstruction is the most common cause of urinary tract obstruction in infants and children. It is believed to result from various causes, including: 1) abnormal development of the proximal ureteral smooth muscle; and 2) aberrant vessels, adhesions, or bands crossing the upper ureter and renal pelvis. It is commonly initially identified on prenatal imaging, but children with this condition may present at any age. Clinical findings include abdominal pain, flank pain, hematuria, or urinary tract infection. Sonography is the initial diagnostic examination in children with suspected UPJ obstruction. The sonographic findings include dilatation of the intrarenal collecting system (renal pelvis and calyces) without ureteral dilatation (Figure 3).3 The obstruction is bilateral in one-fourth to one-third of patients. Renal parenchymal thinning due to secondary scarring or renal dysplasia may also be seen. The condition may be associated with vesicoureteral reflux; therefore, the imaging evaluation of these children should include VCUG. The diagnosis of UPJ obstruction is confirmed with diuretic renal scintigraphy. The examination shows delayed renal isotope excretion.
Renal vein thrombosis
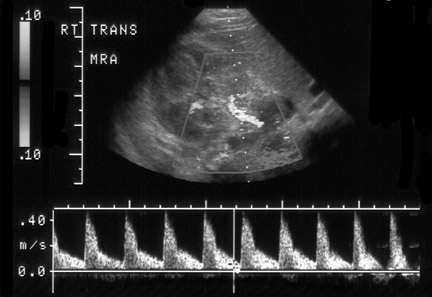
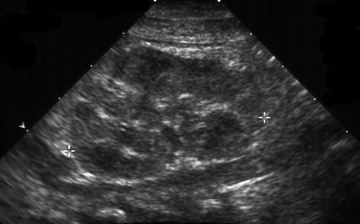
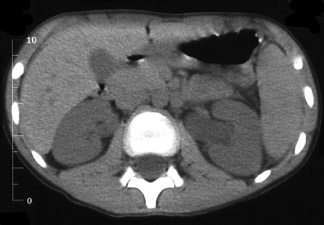
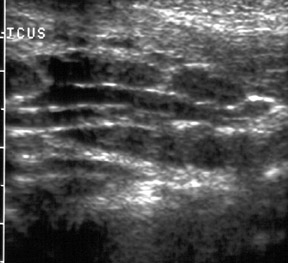
Renal vein thrombosis most commonly presents in young infants, although it can occur at any age. In infants, it is typically associated with hemoconcentration associated with dehydration, sepsis, and maternal diabetes mellitus and is believed to start in the arcuate and interlobar venules, with progression to the hilum. It may also be seen in patients in this age group (in association with indwelling umbilical venous catheters) who develop thrombi in the inferior vena cava. In older children, it is associated with renal tumor, glomerulonephritis, or nephrotic syndrome and is believed to originate in the main renal vein. The clinical presentation includes a palpable mass representing an enlarged kidney, renal insufficiency, hematuria, or hypertension. Doppler sonography is the examination of choice for the evaluation of suspected renal vein thrombosis. The sonographic findings associated with renal vein thrombosis vary depending on the extent and duration of renal venous occlusion. Sonographic findings include the presence of echogenic filling defects in the main renal vein and absence or diminution of renal venous flow surrounding the thrombus.4 The venous outflow obstruction results in diminution of ipsilateral renal arterial flow, resulting in narrowing of the systolic peak and reduction or reversal of diastolic flow with an elevated resistive index in the ipsilateral renal artery (Figure 4).5 Enlargement of the involved kidney with diffuse increase in parenchymal echogenicity or loss of corticomedullary differentiation is also typically seen in the acute period (Figure 5). During the following 7 to 14 days, the renal parenchymal echogenicity in the involved kidney gradually becomes heterogenous and renal size diminishes.
Urolithiasis
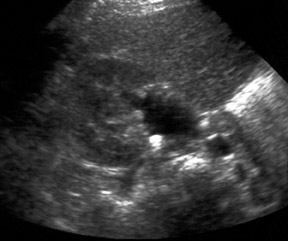
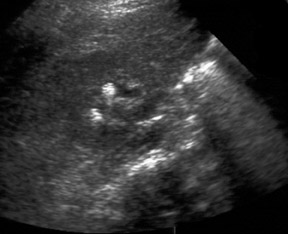
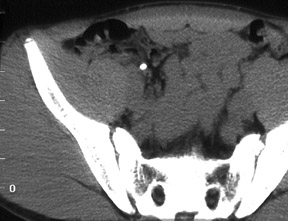
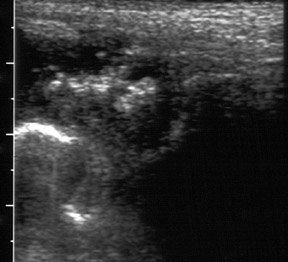
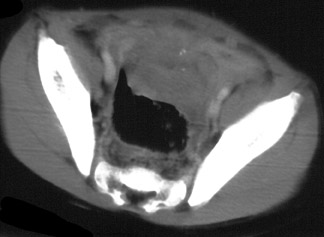
Urolithiasis is a complication of many different disorders. The most common causes of urolithiasis in children are urinary tract obstruction, infection, and bladder augmentation in children with a neurogenic bladder. A majority of urinary tract calculi are composed of calcium mixed with oxalate, phosphate, or a combination of the two. Calculi may also be composed of struvite, cystine, and uric acid. The staghorn is a special type of calculi in which the calculus resembles a stag's antlers and is composed of calcium, magnesium, ammonium, and phosphate. They are typically large and have a laminated appearance. Children with urolithiasis present with severe flank pain or hematuria. Generalized symptoms may be noted if a secondary urinary tract infection develops. The primary imaging modalities for the evaluation of urolithiasis are sonography and computed tomography (CT). Sonography is highly accurate for the diagnosis of calculi within the intrarenal collecting system and the bladder (Figure 6).6 However, it is relatively insensitive in the assessment of ureteral calculi. Associated acoustic shadowing is noted at sonography with calculi >5 mm. However, smaller calculi may not shadow. Dilatation of the urinary collecting system proximal to the calculus may be noted if there is associated partial urinary tract obstruction (Figure 7). Sonography is also useful in the follow-up assessment of children with calculi to follow the response to therapy. Unenhanced CT has been shown to have the highest sensitivity in the diagnosis of urolithiasis. In children with acute flank pain in whom the diagnosis is uncertain, it can accurately determine the presence of renal, ureteral (Figure 8), or bladder calculi (Figure 9).7,8 Additionally, CT also allows for the assessment of extra-urinary causes of acute flank pain. CT for the detection of urolithiasis can be performed at low mAs (30 to 60 mAs) due to the high tissue contrast involved, thus decreasing patient radiation dose.9
Infected urachal remnant
The urachus is an allantoic remnant located in the midline between the umbilicus and the dome of the bladder. The urachal lumen is typically obliterated during fetal life or early in the neonatal period, and the remnant is reduced to a fibrous cord. Occasionally, there is failure of all or a portion of the urachal lumen to be obliterated. Such abnormalities are characterized as urachal remnant abnormalities, including: 1) patent urachus, 2) urachal sinus, 3) urachal diverticulum, and 4) urachal cyst.10,11 Urachal remnants may become infected, resulting in enlargement of the structure with abscess formation. The patients typically present with acute abdominal pain, fever, and leukocytosis. At cross-sectional imaging with sonography or CT, a complex midline mass is noted between the umbilicus and the dome of the bladder (Figure10,11 A tubular component can usually be identified that allows for differentiation of infected urachal remnants from other causes of intra-abdominal abscesses (Figure 11). CT may provide improved definition of the extent of abscess and enhanced delineation of the anatomic relationship of the abscess to the bladder (Figure 12). The treatment of an infected urachal remnant typically involves surgical drainage.
Hemorrhagic cystitis
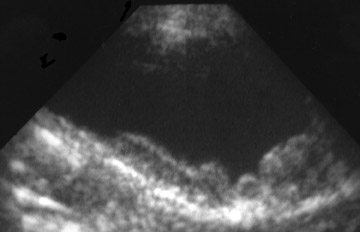
Hemorrhagic cystitis results from damage to the bladder transitional epithelium resulting in diffuse bleeding. The etiology may be multifactorial. The condition has been associated with drugs, infection, and toxins. Chemotherapeutic agents, particularly cyclophosphamide and busulfan, are the drugs most commonly associated with the condition. It has been frequently reported following bone marrow transplantation, particularly in younger children.12 Children with hemorrhagic cystitis typically present with gross hematuria, dysuria, suprapubic pain, and urinary frequency. The extent of hemorrhage may be severe and the condition may be life-threatening. It can result in impaired renal and bladder function and may require multiple transfusions. Sonography is usually the initial modality in the evaluation of suspected hemorrhagic cystitis. Associated sonographic findings include focal (Figure 13), multifocal (Figure 14), or circumferential bladder wall thickening.12-14 The bladder wall thickness should not exceed 3 mm for a distended bladder or 5 mm for a nondistended bladder.15 When the bladder wall thickening is focal, it may resemble a bladder wall mass. Echogenic clots may also be noted within the bladder lumen. The bladder may have a reduced capacity. In severe cases, there may be complete contraction of the bladder without a visualized lumen. There may be associated hydronephrosis secondary to obstruction from bladder clots. In addition, the entire urothelial surface is at risk, and lesions of the renal pelvis and ureter have been reported. Therefore, suburothelial thickening of the renal pelvis may also be noted. Sonography is also a useful modality for the serial evaluation of children with hemorrhagic cystitis for monitoring response to therapy.
Conclusion
Imaging evaluation plays an important role in the diagnosis and management of pediatric urinary tract emergencies. Selection of the appropriate imaging strategy and knowledge of the typical imaging findings associated with these conditions is essential to ensure prompt diagnosis and treatment.
References
REFERENCES
- Macpherson RI, Leithiser RE, Gordon L, et al. Posterior urethral valves: An update and review. RadioGraphics.1986;6:753-791.
- Cohen HL, Susman M, Haller JO, et al. Posterior urethral valve: Transperineal US for imaging and diagnosis in male infants. Radiology. 1994;192:261-264.
- Brown T, Mandell J, Lebowitz RL. Neonatal hydronephrosis in the era of sonography. AJR Am J Roentgenol. 987;148:959-963.
- Helenon O, Rody FE, Correas J-M, et al. Color Doppler US of renal vascular disease in native kidneys. RadioGraphics.1995;15:833-854.
- Laplante S, Patriquin HB, Robitaille P, et al. Renal vein thrombosis in children: Evidence of early flow recovery with Doppler US. Radiology. 1993;189:37-42.
- Haddad M, Sharif HS, Shahed MS, et al. Renal colic: Diagnosis and outcome. Radiology. 1992;184:83-88.
- Smith RC, Verga M, McCarthy S, et al. Diagnosis of acute flank pain: Value of unenhanced helical CT. AJR Am J Roentgenol. 1996;166:97-101.
- Sommer FG, Jeffrey RB, Rubin GD, et al. Detection of ureteral calculi in patients with suspected renal colic: Value of reformatted noncontrast helical CT. AJR Am J Roentgenol. 1995;165:509-513.
- Tack D, Sourtzis S, Delpierre I, et al. Low-dose unenhanced multidetector CT of patients with suspected renal colic. AJR Am J Roentgenol. 2003;180:305-311.
- Khati NJ, Enquist EG, Javitt MC. Imaging of the umbilicus and periumbilical region. RadioGraphics. 1998;18:413-431.
- DiSantis DJ, Siegel MJ, Katz ME. Simplified approach to umbilical remnant abnormalities. RadioGraphics.1991;11:59-66.
- Benya EC, Sivit CJ, Quinones RR. Abdominal complications after bone marrow transplantation in children: Sonographic and CT findings. AJR Am J Roentgenol. 1993;161:1023-1027.
- Yang CC, Hurd DD, Case LD, et al. Hemorrhagic cystitis in bone marrow transplantation. Urology. 1994; 44:322-328.
- McCarville MB, Hoffer FA, Gingrich JR, et al. Imaging findings of hemorrhagic cystitis in pediatric oncology patients. Pediatr Radiol. 2000;30:131-138.
- Jequier S, Rousseau O. Sonographic measurements of the normal bladder wall in children. AJR Am J Roentgenol. 1987;149:563-566.
Related Articles
Citation
Pediatric urinary tract emergencies. Appl Radiol.
June 4, 2004